
The Zen program provides a relaxing sound background so adult hearing aid wearers may use it for relaxation in quiet where listening to the environment and/or speech is not critical. In the hands of those who are trained in tinnitus management, this may be a convenient and discreet sound therapy tool for hearing-impaired people with tinnitus. The following survey was conducted to determine if indeed clinicians who were trained in tinnitus management would find the Zen program useful for their tinnitus patients.
In a previous article,1 we reviewed the concept of using music on relaxation and stress reduction. We also reported on a study to demonstrate the relaxation properties of some fractal-generated musical chimes used in the Zen program. In this article, we report on the results of a survey on the use of such music for tinnitus management in clinics.
Tinnitus and Music
The limbic system is known to be associated with emotions. However, it is also highly involved in music processing. Different types of music—major vs minor keys, fast vs slow tempo, etc—have been shown to activate different parts of the limbic system2,3 and may alter the levels of certain neurotrophins in the hypothalamus. These changes in the concentration of neurotrophins could also lead to a reduced stress response.4 Subsequent changes in heart rate and respiration rate may also result.5

|

|

|
| This article was submitted to HR by Francis Kuk, PhD, director of audiology, and Heidi Peeters, MA, and Chi Lau, PhD, who are research audiologists at the Widex Office of Research in Clinical Amplification (ORCA USA) located in Lisle, Ill. Correspondence can be addressed to Francis Kuk, PhD, at . | ||
In recent years, research on the origin of tinnitus and the emotional distress associated with it suggests that tinnitus results from the peripheral attenuation of auditory input.6 This attenuation provokes an increase in central auditory system activity from the dorsal cochlear nucleus through the auditory cortex, as well as a coupling with the limbic system (particularly the hippocampus and amygdala) via collateral connections from the thalamus and other structures.7 Stimulation of the thalamus results in a release of neurotransmitters—including adrenaline—to produce an autonomic nervous system response associated with stress.
Because tinnitus is associated with a decreased peripheral stimulation and an alteration of limbic system activity (stress), one may manage tinnitus effectively by increasing the peripheral activity and/or altering the activity of the limbic system. The former can be achieved through the use of appropriate amplification. The latter may be achieved through the use of relaxation and de-stressing activities.
Both of these goals may be achieved if current personal hearing aids are able to generate soothing music that can be used for relaxation. In this way, the person with hearing impairment can continue to receive appropriate peripheral auditory stimulation and, when appropriate, activate the music for relaxation/tinnitus management.
A Hearing Aid That Generates Music
A hearing aid (mind440) with a relaxing music program (called the Zen) has been introduced. This hearing aid uses a Dual Integrated Signal Processing (Dual-ISP) platform with 15 channel enhanced dynamic range TruSound compression.8 The Zen program generates music based on an understanding of the optimal music characteristics for relaxation using a patented fractal algorithm. The Zen music is composed of tonal notes with an overall chime or bell-choir quality. The use of fractals results in tones that do not repeat themselves. This assures the novelty of the generated music and allows for aesthetically pleasing sounds.
There are 5 pre-defined Zen styles or patterns called aqua, coral, green, lavender, and sand—each having a unique combination of tonal pitch, tempo, and intensity based on the in situ hearing loss of the wearers. Each music style can be further adjusted on its volume, pitch, and tempo to produce the most desirable (or relaxing) sound for the wearer. The level of the Zen tones also adjusts automatically to be above the level of the ambient noise in the environment.
Zen music may be played in addition to conventional amplification (Zen + HA), or it may be played alone with the hearing aid microphones turned off (Zen alone). In addition, it may be played along with a low-level broadband noise background with the hearing aid microphone “on” (Zen + HA + noise). These programs are accessible through a program button or a remote control.
The Zen program provides a relaxing sound background so adult hearing aid wearers (>21 years) may use it for relaxation in quiet when listening to the environment and/or speech is not critical.1 In the hands of those who are trained in tinnitus management, this may be a convenient and discreet sound therapy tool for people with hearing loss and tinnitus. The current survey was conducted to determine if indeed clinicians who were trained in tinnitus management would find the Zen program useful for their tinnitus patients.
Study Methods
Procedure. A survey on the use of Zen for tinnitus was sent to all Widex customers who had ordered the mind440. The letter specifically requested responses only from clinicians who were trained in tinnitus management and who used the mind440 and/or the Zen program for tinnitus management. (It should be noted that Zen had not previously been promoted for tinnitus remediation.) The announcement and link to the survey were posted on Widex’s Web site as well.
|
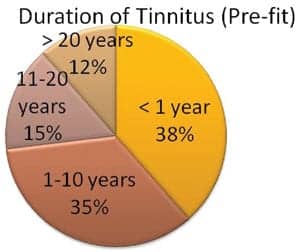
| FIGURE 1. Pie chart showing the distribution of reported tinnitus duration prior to treatment. |
The duration of survey collection was 6 months. Customers who had used the mind440/Zen and those who intend to use the mind440/Zen in the next 6 months were asked to complete a survey for each patient and return the survey via fax, e-mail, or mail to Widex. The survey was intentionally made brief (<5 minutes to complete) so there was a higher chance that the clinicians would complete and return it. No compensation or incentive was provided to the clinicians (and their patients) for completing the survey.
Participants. A total of 49 surveys regarding individual tinnitus patients were returned by 25 clinicians. Of these surveys, 43 surveys returned by 17 clinicians included data on the use of mind440/Zen for tinnitus treatment. Surveys were returned from throughout the United States and from one clinician in Canada. A list of these clinicians and their affiliations is included in the Acknowledgement section in the online version of this article. All clinicians who completed the surveys had at least 1 year of experience treating tinnitus, with the exception of one survey that was completed by a fourth-year AuD student on an externship. Hearing loss degree ranged from borderline/mild hearing loss to moderate-severe to profound. Of the 43 surveys, 3 of the patients had a unilateral hearing loss. For the remaining 40 patients with bilateral hearing loss, 32 had a symmetrical configuration and 8 had an asymmetrical hearing loss.
Overall Survey Results
|
| FIGURE 2. Rated severity of tinnitus (percentage of respondents) at pre- (baseline) and post-fitting of Zen. |
Clinician experience and training. The majority of clinicians (82%) who returned the survey reported having at least 3 years of experience treating tinnitus. A total of 13 of the 17 (77%) also reported completing formal courses on tinnitus treatment that included Tinnitus Retraining Therapy (TRT) and other approaches, such as Cognitive Behavioral Therapy (CBT). In total, 13 clinicians reported data on only one patient, 3 clinicians reported data on 2 to 4 patients, and one clinician reported data on 18 patients.
Tinnitus duration. The duration of tinnitus prior to the initial contact ranged from 2 weeks to 40 years: 38% of the patients had tinnitus for less than 1 year; a total of 35% of the patients had tinnitus that lasted between 1 and 10 years, 15% of the patients had tinnitus that lasted between 11 and 20 years, and 12% had tinnitus for more than 20 years (Figure 1).
Tinnitus quality. The sound quality of the tinnitus varied among patients at initial contact. Ringing occurred in 42% of the patients. Hissing was reported in 23% of cases. Roaring occurred in 6% of the patients, and pulsing was reported by 2% of the patients. Other tinnitus qualities (27% of patients) included whining, whistling, crickets, buzzing, shushing, humming, sizzling, and whooshing. Quality of the tinnitus was not changed after the treatment (unless it completely disappeared).
|
| FIGURE 3. Percentage of patients who had access to each program type. |
Tinnitus location. Prior to treatment with the mind440, 59% of patients reported tinnitus in both ears, 17% reported tinnitus in the left ear only, and 12% reported tinnitus in the right ear only. The remaining 12% reported tinnitus located in the middle of the head. Tinnitus location did not change from treatment (other than a complete disappearance in some cases).
Tinnitus severity. The severity of the patient’s tinnitus was rated on a 5-point scale ranging from mild to profound during the pre- and post-Zen fitting sessions. Figure 2 shows the number of respondents in each rating category, plotted as a percentage. Only those subjects (n=35) who had ratings on both pre- and post-fitting were included in the analysis. During the pre-fitting, the median tinnitus severity was “moderately severe”; during postfitting, the median severity was “mild.” Of the 35 patients, 5 who reported either mild or moderate tinnitus did not change the rated severity of their tinnitus. A Wilcoxon signed rank test showed that post-fitting ratings were significantly better than baseline (Z=4.78, p<0.001).
Zen and Hearing Aid Options in Tinnitus Treatment
There were 7 hearing aid options utilized for tinnitus management. Results showed that most patients were given “HA + Zen” (55.3%), followed by “HA + Zen + Noise” (48.9%). Less than 10% of patients were given “Zen alone,” “Zen + Noise,” “HA + Noise,” and/or “Noise alone.” Six patients reported improvements on tinnitus measures, which were a direct result of mind440 hearing aid use.
|
| FIGURE 4. Scatter-plot of TRQ scores obtained at baseline vs last follow-up session for individual patients. Those points falling under the blue dashed line indicate improvement of 20 points or greater. |
The fact that the majority of the clinicians chose to use the Zen (and/or noise) with the hearing aid deserves mention. First, it suggests that the option of continuous Zen does not affect the patient’s ability to communicate in their daily lives. Second, it questions the validity of tinnitus treatment options that interrupt the patients’ listening of the treatment stimulus because the sound therapy tool does not include a hearing aid option. The third point—perhaps a reflection of the training of those clinicians completing the survey—is that most of these cases were fitted on the principle of “set and forget” as advocated by the TRT principles.9 Having the Zen stimuli available along with the hearing aid provides the continuous stimulation for both the acoustic needs (amplification) and relaxation needs of the tinnitus patients.
Effectiveness on TRQ
The Tinnitus Reaction Questionnaire (TRQ)10 is commonly used by clinicians who conduct tinnitus management. The absolute scores on the TRQ ranged from 0 to 104 with a higher score indicating greater tinnitus severity. Of the 43 patients who reported, only 26 patients had both pre-fit and post-fit TRQ scores. Figure 4 shows the scatter-plot of TRQ scores for pre-fit (baseline) and post-fit (the last follow-up session). A total of 31% of patients (ie, 8 patients) had TRQ improvement within 20 points, and 69% of patients (ie, 18 patients) had improvement greater than 20 points (indicated by the blue dashed line). One patient had improvement of 91%. Pre-fitting TRQ scores ranged from 3 to 91 while post-treatment scores ranged from 0 to 47.
Potential Factors Affecting Tinnitus Improvement
|
| FIGURE 5. Improvement of TRQ scores re clinician’s tinnitus treatment experience. |
|
| FIGURE 6. Improvement of TRQ scores re Zen default or adjusted settings. |
|
| FIGURE 7. Improvement of TRQ scores re tinnitus rating in pre-fitting. |
The current data set provides a glimpse of the factors that may affect tinnitus benefits. Figure 5 shows the TRQ improvement as a function of the number of years the clinicians had treated tinnitus patients. Only those clinicians who provided an exact number of years were included. To distinguish the clinician who reported 18 patients from the other clinicians, we identified her as “Clinician 7” and marked her responses with a pink triangle. As one can see, there did not appear to be a relationship between TRQ improvement and clinician experience. Furthermore, there was not a difference in TRQ benefit between using the hearing aids as “HA + Zen” and “HA + Zen + noise.”
We also compared the amount of tinnitus improvement on the TRQ between the cases fitted with the default Zen settings and those with the adjusted Zen settings. Figure 6 shows that in a majority of cases the clinicians adjusted the Zen settings. Only three used the default setting. This makes any conclusion on the adequacy of the default setting difficult. What is interesting to note is that, even with the adjustment on the Zen settings, there was a wide spread of tinnitus benefit reported on the TRQ. This highlights the need for individual adjustment of the parameters for optimal performance.
Figure 7 shows TRQ improvement as a function of baseline tinnitus severity. Not surprisingly, those with a more severe tinnitus showed more improvement on the TRQ. This highlights the effectiveness of the Zen for all degrees of tinnitus severity and not just for a mild or severe tinnitus. In a separate analysis, we have also determined that the duration of the tinnitus did not correlate with the amount of tinnitus improvement. This again supports the broad use of the Zen program for all tinnitus patients regardless of how long they have been affected by their tinnitus.
Discussion
The results of the survey showed that the mind440 hearing aid with Zen was effective in the hands of experienced clinicians in managing their tinnitus patients. Indeed, an overwhelming 87.5% of the respondents reported a decrease in tinnitus severity with the use of the Zen program, either alone with the HA, or in combination with the HA and the broadband noise. This suggests that the Zen could be an effective sound therapy tool for clinicians to use in their tinnitus management programs.
While the Zen program is shown to be effective, one must remember that the majority of the respondents in this survey were experienced and trained clinicians in tinnitus management. One recalls that the majority had over 3 years of experience treating tinnitus, and many also received formal training in tinnitus management such as Tinnitus Retraining Therapy (TRT), Behavioral Cognitive Therapy, or tinnitus training by a commercial entity (eg, Neuromonics). These respondents were familiar with the ingredients for success in tinnitus management. They realized that success depends on a combination of optimal fitting of the hearing aids, choice (and adjustment) for a good sound therapy tool, counseling, and proper expectation and follow-up. Indeed, the diversity of the hearing aid option used (ie, Zen + HA, Zen + HA + noise), the various Zen styles chosen (aqua vs green, etc), and the fact that the majority had adjusted the Zen parameters suggest that the Zen program has the flexibility to meet the diverse preference of tinnitus patients. It also suggests that competence of the clinician is necessary to bring about positive change.
The same result may not be evident when the Zen is in the hands of an inexperienced clinician. One needs to realize that the Zen is a useful sound therapy tool that offers a discreet and convenient musical chime for relaxation/tinnitus purposes. The tool itself is neither good nor bad; its goodness depends on how well the tool is used. In that regard, clinicians who intend to use the Zen for their tinnitus patients should have received training on tinnitus management prior to use of the Zen option.
ADDITIONAL READING:
![]()
“Tinnitus Treatment and the Effectiveness of Hearing Aids: Hearing Care Professional Perceptions,” by Sergei Kochkin, PhD, and Richard Tyler, PhD, in December 2008 issue of HR. You can also listen to a PODCAST with these authors.
As surveys go, it is difficult to control all the potential variables. One is the potential of the placebo effect. One may argue that, since this is a typical clinical encounter, the mere fact that the patient was properly counseled by the clinicians would have reduced a majority of the tinnitus complaint. Indeed, counseling is a major part of tinnitus management.9 Adding to the fact that 6 of the 43 patients actually reported a decrease in tinnitus severity with the use of the mind440 hearing aid alone (without Zen) could argue that the mind440 by itself may be sufficient. Hearing aids have been reported to reduce tinnitus severity in inflicted individuals.11
While these possibilities are real, it is noteworthy that, in a separate study,12 the authors were able to show differential preference for the different Zen styles and the differential effectiveness between the hearing aid alone condition and the hearing aid plus Zen (or plus noise) condition in patients with long-standing tinnitus. This suggests that the effectiveness of the Zen is not simply due to the benefit of hearing aids or counseling alone, but rather a combination of hearing aids, counseling, and optimal Zen use.
Conclusions
1) 100% of the patients who completed the pre- and post-TRQ questionnaire reported a reduction in tinnitus.
2) 85.7% of those patients who reported pre- and post-tinnitus severity reported a reduction in tinnitus severity.
3) The “HA + Zen” and “HA + Zen + Noise” program options were most frequently provided to address tinnitus.
4) Zen aqua was recommended the most frequently as the preferred Zen style.
Acknowledgements
We thank the following clinicians (and their facilities) for completing the surveys reported in this paper. They are:
Beth Alberto, AuD
Hearing Care of Summerville, SC
Jennifer Auer, AuD
Audiology by the Sound, NY
Manuel Cohen & Deb Lynn
Arden Hill Speech and Hearing, NY
Melissa Ferrello, AuD
Fairview Audiology Clinic, MN
Heidi S. Frazier, MS
Midwest Ear Institute, MO
Anne Giroux, AuD
Anne Giroux Audiology, ME
Melanie Herzfeld, AuD
Woodbury, NY
Kristi Hesse
Arizona Hearing Specialists, AZ
Amanda Jones, AuD
Nashville ENT Audiology, TN
Scott Laidman, HIS
Helix Hearing Care Centre, ON, Canada
Gladys Larson, MA, FAAA
Johnson County Healthcare Center, WY
Randa Mansour-Shousher, AuD
Northwest Ohio Hearing Clinic, OH
Sol Marghzar, AuD
The Hearing Doctor, CA
Brae Mc Dougald, MA
Lakeview Hearing Center, TX
Jan Miller, AuD
Hearing & Speech Associates, Inc
The Plainview Hearing Center, NY
Megan Nightingale
Peninsula Hearing, Inc, WA
Melissa Palmer
High Point Audiological, Inc, NC
Jennifer Peterson
OHSU Tinnitus Clinic, OR
Ryan Pratt, AuD
Ohio University Therapy Associates, OH
John Risey
Ochsner Clinic, LA
Paula Schwartz, AuD
Audiology Concepts, Inc, MN
Chris Stocking, AuD
University at Buffalo, NY
Hearing Rehab Center Inc, CO
Suburban Audiology Center, PA
References
- Kuk F, Peeters H. Hearing aids as a music synthesizer. Hearing Review. 2008;15(10):28-38. Accessed August 18, 2010.
- Weinberger N. Music and the brain. Scientific American. 2004;291(5):88-95.
- Mitterschiffthaler M, Fu C, Dalton J, Andrew C, Williams S. A functional MRI study of happy and sad affective states induced by classical music. Hum Brain Mapp. 2007;28(11):1150-1162.
- Angelucci F, Ricci E, Padua L, Sabino A, Tonali P. Music exposure differentially alters the levels of brain-derived neurotrophic factor and nerve growth factor in the mouse hypothalamus. Neurosci Lett. 2007;429(2-3):152-155.
- Brunges M, Avigne G. Music therapy for reducing surgical anxiety. Clin Innov. 2003;78(5):816-818.
- Kaltenbach J. The dorsal cochlear nucleus as a participant in the auditory, attentional and emotional components of tinnitus. Hear Res. 2006;216-217:224-234.
- Eggermont J, Roberts L. The neuroscience of tinnitus. Trends in Neuroscience. 2004;27(11):676-682.
- Kuk F, Jessen A, Baekgaard L. Ensuring high fidelity in hearing aid sound processing. Hearing Review. 2009;16(3):34-43.
- Henry J, Trune D, Robb M, Jastreboff P. Tinnitus Retraining Therapy: Clinical Guidelines. San Diego: Plural Publishing; 2007.
- Wilson P, Henry J, Bowen M, Haralambous G. Tinnitus Reaction Questionnaire: Psychometric properties of a measure of distress associated with tinnitus. J Speech Hear Res. 1991;34:197-201.
- Kochkin S, Tyler R. Tinnitus treatment and the effectiveness of hearing aids: hearing care professional perceptions. Hearing Review. 2008;15(12):14-18. Accessed August 18, 2010.
- Sweetow R, Henderson-Sabes J. Effects of acoustic stimuli delivered through hearing aids on tinnitus. J Am Acad Audiol. August 2010. In press.
Citation for this article:
Kuk F, Peeters H, Lau CL. The efficacy of fractal music employed in hearing aids for tinnitus management. Hearing Review. 2010;17(10):32-42.



