Inside the Research | April 2017 Hearing Review
This month, we wanted to turn our attention to an annual conference each June that is celebrating its 25th anniversary in 2017: The International Conference on Management of the Tinnitus and Hyperacusis Patient held each year at the University of Iowa in Iowa City and organized by Richard Tyler, PhD.

Richard Tyler, PhD
Beck: Good Morning, Rich. It’s always great to spend a few moments with you.
Tyler: Thanks Doug. I appreciate your time, too.
Beck: My pleasure. I might as well start by congratulating you on the 25th Annual International Conference on Management of the Tinnitus and Hyperacusis Patient that will be held June 15 and 16th in Iowa. And, of course, while we’re on the subject, please tell me how and why you launched the project a quarter of a century ago!
Tyler: Thanks Doug. Well, 25 years ago there weren’t any venues for clinicians and researchers to share knowledge about tinnitus. As you may recall, patients were told to get used to it, and they were told nothing could be done. As a result, clinicians avoided tinnitus patients, and scientists were not aware of the need for tinnitus research. In 1992, I started the conference for clinicians and scientists to come together so that they could learn from each other. Since that time, every year, selected clinicians and scientists offer presentations to inform and learn from each other. I organize it in such a way that all important topics are covered so that attendees will go back with a firm understanding of how they can help their patients.
Beck: And, I think it’s fair to say your conference has been the most important annual tinnitus conference across the globe, from which a from which a vast quantity of important books, questionnaires, articles, and information has arisen.
Tyler: Thanks again. We got a foothold when there simply was no competition. We established a comprehensive format covering established and novel procedures. We carefully select the Guest of Honor each year, and include a diverse range of speakers to cover all areas related to current and future treatments, as well as novel approaches to understanding the mechanisms and outcomes related to the patients, and their diagnosis and treatment options. This year, we’ll have two days of presentations [see sidebar].
Beck: Thanks Rich. Maybe it’s just me, but it seems like we’ve had a resurgence of interest in tinnitus in the last five years. Is that correct?
Tyler: I think so. When you go back only 10 or 15 years, we had some useful tools for the tinnitus patients, and we had maybe five or six companies interested in producing those same tools. But frankly, after a few years’ time, some of them backed out, and I think that was primarily because we didn’t have enough knowledge about, or access to, counseling tools specific to the needs of the tinnitus patent. But as we fast forward to 2017, many patients have benefitted from excellent hearing aid fittings and counseling developed to meet the individual needs of the tinnitus patient.
Beck: And so, what crosses your mind when you still hear things professionals say like “Everyone has tinnitus, you just need to get used to it” and “There’s nothing that can be done to help”?
Tyler: Well, when I hear those statements, it’s clear to me the people who make those statements are totally out of touch with the reality of tinnitus evaluation and treatment.
Beck: And, as you know, our friend and colleague Robert Sweetow, PhD, stated a few years ago something along the lines of…“it’s unethical and arguably immoral to tell a tinnitus patient ‘there’s nothing that can be done to help.’” I absolutely agree with Dr Sweetow and I often state and write the same thing. In my opinion, I believe we can help some 90% of all tinnitus patients manage their tinnitus. Would you agree?
Tyler: Absolutely, and I am so pleased so many are now interested in helping tinnitus patients and are preparing themselves. Most people with tinnitus will benefit from sound therapy devices, hearing aids, and even just knowing that you care and that you’re there to help. Just knowing they have options and advocates is therapeutic as the patients realize they’re not in this alone.
Beck: OK, I appreciate that. Please tell me your thoughts on Cognitive Behavioral Therapy (CBT). In my review of the literature, it’s clear that CBT offers a systematic management protocol, and of note, CBT was introduced to most of us by Dr Sweetow. CBT appears to offer impressive non-audiologic alternatives for patients who don’t benefit from audiology-based solutions.
Tyler: Sure, CBT is a fairly standard protocol that, depending on the situation, does have many helpful components. However, I do think sometimes it is overemphasized. As my colleague from Denmark, psychologist Anne-Mette Mohr, has pointed out, it is really important to understand where the individual patient is at. Using a prescriptive formula for treatment for everyone is not always the best. Treatments can help people accept their tinnitus, not fight it and control it. Also the compentency and commitment of the therapist is one of the most important ingredients.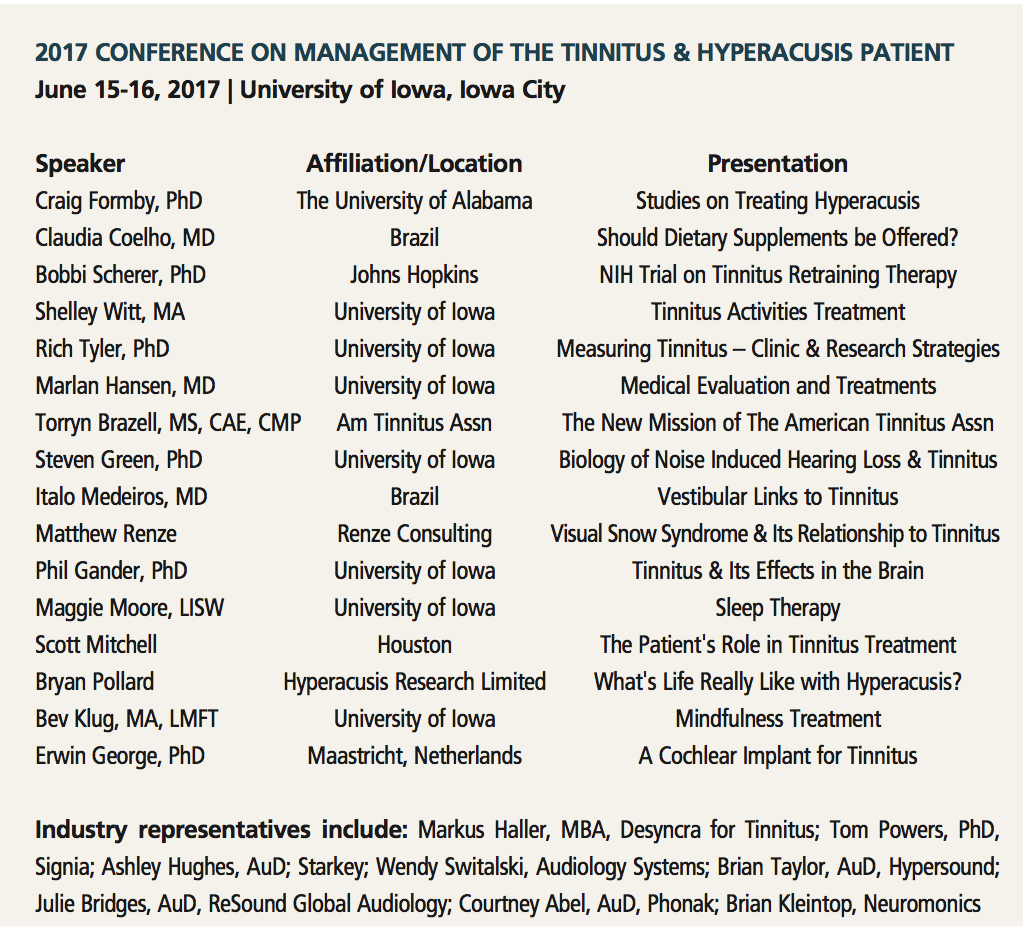
As you know, Doug, we use the Tinnitus Activities Treatment (TAT) program, and it’s a progressive program. It focuses on individual interactive counseling, based on the four primary functions affected by tinnitus: thoughts and emotion, hearing, sleep, and concentration. It is used widely; clinicians can download the pictures and adapt them to their own needs [visit: https://medicine.uiowa.edu/oto/research/tinnitus-and-hyperacusis].
Beck: Rich, please tell me about the Tinnitus Primary Function Questionnaire that was developed by you and your colleagues.
Tyler: Sure. Again, it focused on the four primary functions affected by tinnitus: sleep, concentration, hearing, as well as thoughts and emotions. As we dig deeper, it becomes apparent that some people report it’s difficult to know the difference between the hearing problems from their hearing loss, as opposed to, or compared to, hearing problems caused by their tinnitus. However, most tinnitus patients do have hearing loss. So we can work to help people with their hearing loss, and, of course, as we effectively manage their hearing loss, we often positively impact their tinnitus too.
Beck: OK, fair enough. Let me ask a few specific questions. That is, based on your very significant experience with tinnitus patients, is it generally true that most tinnitus is high frequency, such as greater than 5000 Hz?
Tyler: Yes. In general, that appears to be true. Most tinnitus appears to be in the higher frequencies, and about one-third of all patients experience tinnitus above 5000 Hz.
Beck: And what about the hearing aid’s spectral response being able to match the perceived tinnitus pitch?
Tyler: Intuitively, that seems like a good idea. However, there are many patients for whom a given spectral response through a hearing aid is not as high as the pitch-matched tinnitus, and the hearing aid may offer significant and, perhaps, total tinnitus relief. So, I like having an extended bandwidth available, but it may or may not be useful for a specific patient.
Beck: So sometimes a broader or lower spectral response may be useful for the tinnitus patient?
Tyler: Exactly. Each patient is, more or less, a single-subject study, and we have to approach them each as individuals. That is, we have to have a toolbox which includes multiple tools; what works for one person, may not work for the other. Each patient is different.
Beck: One presentation which has often fascinated me is the patient with a bilaterally symmetric mild-moderate sensorineural loss who reports tinnitus in only one ear. Given that scenario, do you fit the ipsi-lateral ear?
Tyler: It’s interesting you raise that question! I wrote an article with Ruth Bentler in 1987 on this issue, and our recommendations and conclusions seem to hold true today. That is, although it’s logical to start with, and to try to treat the ipsi-lateral ear (and I suspect this is why you asked the question), sometimes you might have to fit the contralateral ear, and, then again, sometimes you have to fit both ears. Sometimes we can mask tinnitus ipsi-laterally, and sometimes contra-laterally, and sometimes not—but the key is to try a device on one or both ears, and see what works best for that specific patient.
As I heard you say in one of your tinnitus lectures, there really are no “go-to” solutions for hearing loss and tinnitus. Each patient is unique, and of course, because you’re working with individuals and their perception, one must be flexible and have a toolbox that includes and allows multiple and various solutions.
Specific to the question you asked, I often find that bilateral hearing aids set to a lower gain setting are very useful. That is, you want to find the lowest level the patient finds acceptable and effective. So it takes time and work, and sometimes trial and error is very useful.
Beck: And, of course, with two devices, the sound can be set to a lower level, and if one attends to spatial cues and delivers a natural acoustic landscape to the ears, it may well be easier for the patient to have amplification in both ears, as using one hearing aid (given a symmetric hearing loss) will tend to present an asymmetric auditory sensation to the patient, and may introduce other, brand-new problems.
Tyler: Absolutely. Again, we have to approach each tinnitus patient as an individual, so we use protocols, tools and trials which lead us to the best solution for that particular patient.
Beck: I agree Rich. Thanks so much for your time today, and I will do my best to get to Iowa this summer. In the meantime, I wish you continued success and an amazing 25th conference, and thanks for all you’ve done to help the tinnitus patient.
Tyler: My pleasure Doug. Thanks again for your interest, too.
MORE DETAILS about the Conference and how to register for it at: https://goo.gl/3ShhQP
Original citation for this article: Beck DL. Tinnitus evaluation and treatment, hyperacusis, and more: An interview with Richard Tyler, PhD. Hearing Review. 2017;24(4):34-35.



