
The authors have developed a Question Prompt List (QPL) that can be used by audiologists to encourage families to engage in both fact-based and adjustment-based questions during audiology appointments. The impetus for developing this QPL was to facilitate more family-centered practices in early intervention.
Pediatrics | November 2017 Hearing Review
A new tool for engaging more families in a child’s hearing management and development
Editor’s Note: As detailed in a June 23, 2017 Hearing Review online news article, Phonak has convened an international expert panel to provide recommendations for Pediatric Family-Centered Audiological Care, marking an expansion of the Phonak Family-Centered Care (FCC) initiative launched in October 2015. The FCC pediatric panel, chaired by Dr Kris English, includes a select group of experts who believe that, in order to provide optimal patient consulting and treatment, audiological care must shift to emphasize both patient and family involvement during the entire treatment process as a means to enhance the value of hearing care services.
Family-Centered Care (FCC) has long been promoted as best practice in the provision of hearing healthcare services for children who are deaf or hard-of-hearing and their families.1,2 Although there is some variation in the definition of FCC among researchers and clinicians, there is consensus in the field of early intervention for children who are deaf or hard-of-hearing that the following 10 best practice principles should be applied:
- Early, timely, equitable access to services;
- Family-provider partnerships;
- Informed choice and decision making;
- Family, social, and emotional support;
- Family-infant interaction;
- Use of assistive technologies and supporting means of communication;
- Qualified providers;
- Collaborative teamwork;
- Progress monitoring; and
- Program monitoring.3
In many ways, the early, timely, and equitable access to services for families of children who are deaf or hard-of-hearing has been facilitated by the widespread implementation of universal newborn hearing screening. Diagnosis is only the first step, however, as once a child’s hearing loss is identified, families have to navigate an often complex system to identify what happens next in their journey. Subsequent and intensive early intervention (EI) is essential, but—unlike screening—not universal. It has been estimated that only about two-thirds of babies diagnosed with hearing loss in the United States receive EI services,4 and, unfortunately, many contemporary EI programs lack the expertise in working with children with hearing loss.5 Despite these challenges, families are generally able to draw upon their natural resilience, with support from their extended family and community network, to develop a support system, identify and mobilize their resources, and move forward.
In every sense of the term, the pediatric audiologist is part of a family’s support system. Indeed, when EI services are limited or non-existent, the pediatric audiologist may be the only professional support available. The type of support needed is unique to each family. For example, we may observe families struggle to understand the nature of hearing loss and the need to amplify their child’s world. Often families will have no previous experience with hearing loss and may perceive a “disconnect” between the diagnosis and their own observations (for example, their child may respond to some sounds, or parents may see little difference in their child’s behavior, with or without hearing aid use). In these circumstances, our typical strategy is to educate families using hearing loss simulations and hearing aid demonstrations, and provide support from other parents who have experienced a similar journey.
From Janet DesGeorge’s notebook: “It was definitely rough emotionally for us during my son’s first year of life. The several hearing tests he took all indicated a hearing loss, but showed inconsistencies, which made diagnosis frustrating. Since he was too young for us to notice symptoms of being hard-of-hearing, and the fact that he did respond to sound to a certain degree, we weren’t even sure if we believed what the professionals were saying.”
We may also work with families who understand the diagnosis and our recommendations, but could still be described as “stuck,” disengaged, or in some way not yet committed to amplification and intervention. Again, the reasons for these various stages of adjustment will be unique to each family, but could be related to grief and guilt, embarrassment, a sense of inadequacy, lack of support, or conflicting advice from family and friends. When such reactions catch the attention of audiologists, some typical strategies are to provide encouragement, recommend family support groups, connect with deaf or hard-of-hearing adults, and refer to a social worker or family therapist.
Although these strategies are used successfully in some situations, there are limitations to relying on this strategy “tool kit” alone, particularly given the likelihood that families may not share their concerns or questions during our appointments.6 As part of a FCC initiative (described below), we found ourselves challenged to develop a new tool that could change the conventional dynamic from a narrow audiological focus to a broader, more family-centered approach. But we first had to ask ourselves what that new tool would look like, and how the tool could be developed.
“Family-Centered Care” Project
Recently, Singh et al7 published a position paper promoting the application of FCC principles to audiology practices. Although the paper focused on the adult population, it also provided a prompt for pediatric audiologists to consider how we engage children and families in family-centered practices. The authors reviewed the following hypothetical scenarios to determine if they represented shared concerns, and, if so, could we find a means to address them?
Scenario #1. Marta was diagnosed with hearing loss at birth, and immediately fit with hearing aids. Her parents disclose that the hearing loss is much like that of Marta’s mother, which she too has had since birth. The mother was also fit with hearing aids in childhood but discontinued their use years ago, preferring to “get by” without them. Now a teenager, Marta has declared that she would also prefer to “get by” without hearing aids.
Scenario #2. Kim’s family has no history of hearing loss but, for reasons unknown, is not fully committed to Kim’s use of consistent amplification. Perhaps because children tend to imitate their parents, Kim has grown up also uncommitted to optimal hearing.
The members of the Pediatric Expert Circle (the authors) agreed that the profession often experiences challenging situations
like those depicted in these scenarios, and that we need help understanding families’ reservations, doubts, and possible lack of trust. Perhaps the profession could consider a new approach to working with families to address their concerns as early as possible, before patterns of non-commitment become established, as depicted in our scenarios.
How to Engage?
Since there is limited guidance in the audiological counseling literature about how to manage these situations, we sought input from other professions. We interviewed 13 colleagues from 9 professions by asking them first to consider these scenarios and then to answer the following questions:
- How does this situation present itself in your profession?
- How does your profession work with this kind of situation?
- What advice can you offer?
Our interviewees included practitioners in social work, pediatric medicine, pediatric psychology/psychiatry, professional clinical counseling, auditory verbal therapy, speech-language pathology, marriage and family therapy, and early intervention. We learned that these kinds of family situations are common across all of these professions, and that our colleagues’ professional training generally prepares them to actively intervene. Overall, their advice to audiology could be summarized as: Engage with families by talking with them, drawing them out, exploring their issues, and developing a strength-based approach to change.
A New Approach for Audiology: Question Prompt Lists
Although the advice we received from other professions was informative, it also highlighted an inherent limitation: audiologists are not professional counselors. However, audiologists do feel comfortable using tools that help initiate and guide many kinds of difficult conversations (for example, the “tool box” developed by the Ida Institute, www.idainstitute.com). Our research in “communication aid” tools led us to the development of a Question Prompt List (QPL).
What is a QPL? QPLs resemble Frequently Asked Questions (FAQ) information sheets, but focus on asking questions, not providing answers. QPLs are communication aids created to encourage patients and families to actively participate in discussions by inviting them to choose the questions(s) they would like to discuss at any given appointment. Brown et al8 note that “a QPL can successfully encourage patients to ask questions about topics that are known to present significant difficulties during consultation discussions” [p 311]. QPLs have been used in patient care for over 20 years (eg, see Butow et al, 1994)9 across a range of health conditions, and they usually focus on facts. For example:
- Who can develop attention deficit/hyperactivity disorder and how common is the disorder?10
- What caused my chronic kidney disease and how does it affect my day-to-day life?11
- Will the illness (advanced cancer) get worse or spread? What are the treatment options? Do they have side effects?12
- What do palliative care hospitals offer? How do I access services/what is the cost involved?13
Existing QPLs provide helpful models, but, as noted, their questions typically focus on the facts of etiology, genetics, management, treatment, etc. To address our specific counseling challenge in audiology, we saw the need for developing a QPL that includes both fact-based and adjustment-based questions that families might like to ask.
Developing the Childhood Hearing Loss QPL for parents. Like the development of many QPLs (see Sansoni et al, 2014),14 this project began with input from experienced hearing healthcare clinicians (pediatric audiologists and speech-language pathologists) and parents, but we did not stop there. We took three additional steps to obtain parent validation, resulting in a question list that more than doubled the original list developed by clinicians.
- The authors first developed a set of 13 “jump-start” questions drawn from their clinical experiences with families.
- Authors JDG, KM, MPM (United States) and KF (United Kingdom) shared this first version (QPL 1.0) with 21 parents.
- Parent input resulted in an expanded set of questions (n = 49), which were organized into categories/themes for ease of use (QPL 2.0).
- QPL 2.0 was evaluated for reading level ratings using the Flesch-Kincaid reading grade level software,15 with results indicating that the reading grade level of 5.8 met recommended readability standards for patient education materials.16,17
- QPL 2.0 was then reviewed by a second cohort of parents (n = 16).
- Reviewed by EW (United States) and KF (United Kingdom);
- A second round of modifications resulted in QPL 3.0, which consisted of a total of 47 items.
- QPL 3.0 was then shared online using the online Qualtrics survey system. Parents known to the authors were invited to review QPL 3.0 item by item, indicating whether each question should be kept as is, kept with revisions, or omitted. Parents could bypass questions without responding, resulting in a range of final answers as described below.
Results
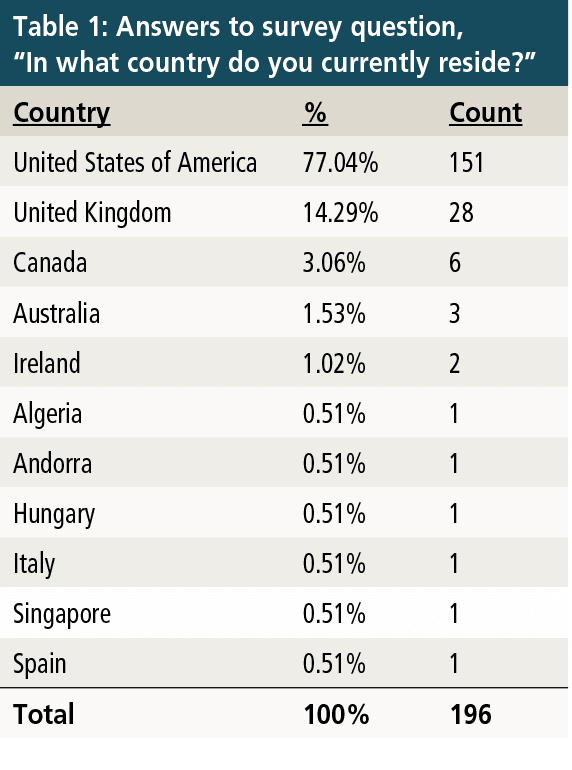
Descriptive data of survey respondents. QPL 3.0 was available online through the Qualtrics survey system for two weeks (August 4-18, 2017). A total of 281 individuals responded to the survey, and 196 volunteered to answer the question, “In what country do you currently reside?” As shown in Table 1, the largest number of responses came from the United States (n = 151) and the United Kingdom (n = 28). Parents indicated that their children who are deaf or hard-of-hearing (n = 184) ranged in age from 2 months to 31 years (M = 7.3, SD = 5.43). Their children’s hearing loss was identified between 1991 and 2017 (n = 162, M = 2010; median = 2012).
A total of 164 parents reported on the type of amplification their child used: 49% (n = 81/164) used hearing aids (HA) only, and 33% used cochlear implants (CI) only (n = 54/164). A smaller percentage (18%; n = 29/164) reported using bone-anchored hearing aids, HA+CI (bimodal), or no amplification.
The majority (56%, n = 92/165) of parents stated that their child relied on spoken language to communicate, followed by a combination of sign and spoken language (38%, n = 62/165). A total of 11 parents (6%) noted that their child relied entirely on sign language, Cued Speech, or gestures as their primary mode of communication.
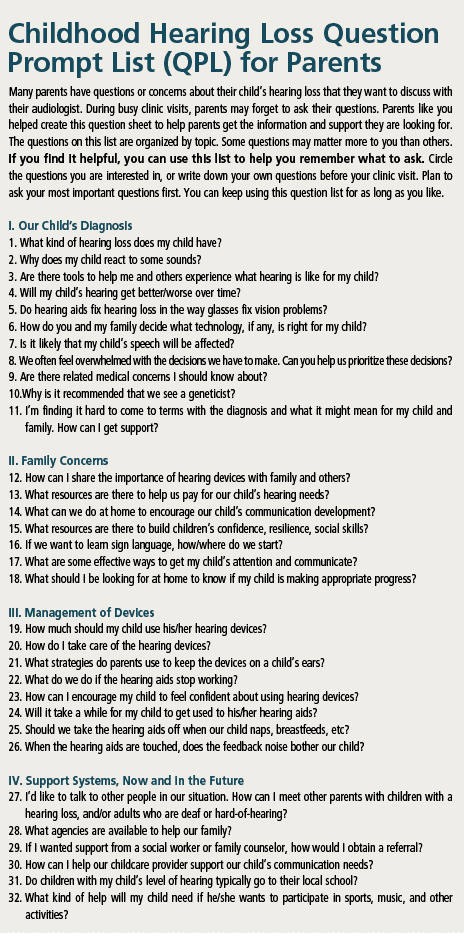
Qualtrics survey results. A total of 47 proposed QPL items were rated by parents within the Qualtrics survey. Parents indicated whether the questions should be kept as is, revised, or omitted. After the authors reviewed the results of the Qualtrics survey, 32 questions were accepted in the final version of the QPL. The authors eliminated questions when 25% or more parents rated them as “omit” or redundant. The final questions covered topics related to early hearing detection and intervention, and were divided into four main topic areas: 1) Our Child’s Diagnosis; 2) Family Concerns; 3) Management of Devices; and 4) Support Systems, Now and in the Future. The final QPL questions are shown in the box titled “Childhood Hearing Loss Question Prompt List (QLP) for Parents.”
Discussion
In this project, we aimed to develop a QPL for families of children who are deaf or hard-of-hearing that could be used by audiologists to encourage families to engage in both fact-based and adjustment-based questions during audiology appointments. The impetus for developing this QPL was to facilitate more family-centered practices in EI. The development of a QPL for parents is certainly in line with the principles of family-centered practice, especially for social and emotional support, and informed choice and decision-making, 2 of the 10 principles promoted by Moeller et al.3
Firstly, the use of a QPL with families provides important social and emotional support by encouraging families to share their questions and concerns about their child’s journey with the audiologist. Parts II and IV of the Childhood Hearing Loss QPL specifically encourage parents to ask questions about their family concerns and available support systems (eg, “If I wanted support from a social worker or family counselor, how would I obtain a referral?”)
Secondly, application of a QPL for this population provides families with the opportunity to ask questions about their child’s diagnosis and EI options (eg, “Will my child’s hearing get better/worse over time?”) and thus facilitates the process of informed choice and decision making, which is a key role of audiologists in the early identification and diagnosis of childhood hearing loss.
To summarize, in contrast with other QPLs, the Phonak Pediatric Expert Circle QPL strived to include areas of both cognitive needs (understanding what is happening) and affective needs (being understood and expressing worries and concerns), as recommended by Bensing and Verhaak.18,19
Limitations. Several limitations are evident in our study. Our initial aim was to develop and validate a tool designed to engage families in their child’s hearing healthcare needs. Although the initial aim has been accomplished, our QPL has not yet been implemented in the clinic with parents of children who are deaf or hard-of -hearing. Further, our expert group of pediatric audiologists initially developed questions based on their experience with parents, which may have inherently introduced some bias into the development of questions. It is important to note, however, that based on comments posted at the end of the survey, the initial two phases of parent review might have minimized this potential bias. Fifty-one parents submitted mostly positive comments, such as:
- Great questions/great project/great resource;
- Great list/I wish I would have had a list like this, and
- Excellent/invaluable/all questions are important/all questions are perfect.
Several parents also proposed additional questions, as well as reminders to avoid leading questions. Others suggested that questions should be framed with an optimistic perspective.
Interestingly, three respondents did not agree that an audiologist should address these questions:
- “A lot of these questions would be better answered by a Child Find (early intervention specialist in the US) aide than an audiologist.”
- “Audiologists are experts in the ear and should refer everything else to H&V (Hands & Voices), DHH EI team, and deaf mentors. Audiologists are biased with technology and that will have a negative impact on families.”
- “Many of the questions are excellent but are better suited for early intervention providers or parent support resources…The advice and information the audiologist provides should be limited to the medical facts of the hearing loss.”
These perceptions may reflect the assigned role of an audiologist in a national healthcare system. If families prefer to limit audiology support to discussion and management of medical and technical issues, that is their right. On the other hand, one parent provided this observation of a more expanded audiologic role (typographical errors corrected): “Often times it’s the audiologists that families pay attention to, therefore audiologists have a unique role in a family’s success.”
Finally, it is evident from parent comments that their perspectives, experiences, and needs vary widely. Thus, there will be diversity in parent questions across and within EI services. For example, some parents could respond that a question is not necessary for the audiologist to address while others feel that the same question identifies a critical need.
Future research. There is a need for future research to explore effective and practical ways to incorporate this tool into the clinical setting. For example, when should the tool be introduced, and how regularly should the QPL be reviewed with families? If the tool is kept on file, it could consistently be referred to, even if different audiologists rotate through family appointments.
In addition, there is a need to explore the relationship of this QPL to knowledge recall, parent satisfaction, and perceived value of audiologic support. As most busy clinics today look for ways to maximize efficiency while providing high-quality service, research into the effect on the length of the audiologist’s consultation time combined with parent satisfaction and quality outcomes will be needed.
Even though this tool was designed for families of young children, we also see the need for additional QPL-type communication aids to help adolescents with the transition into independence,20 and for adults and their family members as they adjust to acquired hearing loss.
Finally, as Sansoni et al14 note, QPLs are not a “substitute for effective communication and cannot ‘fix’ poor communication” [p. v] between audiologists and families. One parent may already have had concerns about effective communication in mind when submitting this query: “Will you offer suggestions for audiologists to [help them] answer these questions?” Our answer is yes. Plans are in development to support audiologists in their engagement with these important conversations.
Conclusion
Interestingly, the Centers for Disease Control and Prevention (CDC) in 2012 published a one-page handout, “Questions You May Want to Ask Your Child’s Audiologist,” as part of a parent education package.21 Although the handout was unknown to 12 of the 13 authors, it may be routinely used in some audiology clinics. Also likely, the handout may be used because families find it on the Internet and bring it to appointments. Just as likely are parents who, although struggling, may not be inclined to take the initiative of finding or generating questions. The goal for our project is to support a more therapeutic dynamic, wherein very early on the audiologist clearly expresses openness to difficult conversations and relationship building, and “walks the walk” by offering a QPL as a starting point.
There is still much work to do, but early parent feedback has been encouraging. As has been shown in the literature, providing a framework for families to ask these or their own questions is the epitome of FCC.
Acknowledgements
The authors thank the following Audiology Doctorate students in the Northeast Ohio AuD Consortium (NOAC) for their assistance with survey development and research: Regan Everiss (University of Akron), Molly Smeal (University of Akron), and Crystal Henry (Kent State University).
Biography: Kris English, PhD, is a professor at the University of Akron/NOAC; Elizabeth Walker, PhD, is an assistant professor in the Department of Communication Sciences and Disorders at the University of Iowa in Iowa City; Kerri Farah, BSc, is the Clinical Lead at Guy’s and St Thomas‘ NHS, UK; Karen Muñoz, EdD, is the Associate Professor of Audiology and Interim Department Head, Communicative Disorders and Deaf Education, at Utah State University; Angela Pelosi, MAuDSA, is the Global Head of Pediatrics at Phonak AG, Switzerland; Nerina Scarinci, PhD, is a Senior Lecturer in Speech Pathology and Audiology at The University of Queensland; Janet DesGeorges is the parent of a deaf daughter and the Executive Director of Hands & Voices, a parent support organization; Holle Aungst, AuD, is the Coordinator of Pediatric Audiology at Head and Neck Institute, Cleveland Clinic; Jane R. Madell, PhD, is a pediatric audiologist, speech-language pathologist, LSLS auditory-verbal specialist, and consults nationally and internationally on managing hearing in children; Mary Pat Moeller, PhD, is Director of the Center for Childhood Deafness, Language and Learning Research at Boys Town National Research Hospital in Omaha, Neb; Josephine Marriage, PhD, is the Director of CHEAR (UK),and is a Clinical Scientist in audiology and registered hearing aid dispenser; Carol Flexer, PhD, LSLS Cert AVT, is a Distinguished Professor Emeritus of Audiology at the University of Akron; Christine Jones, AuD, is the Director of the Phonak Audiology Research Center (PARC) in Warrenville, Ill.

Correspondence to Dr English at: [email protected]
Citation for this article: English K, Walker E, Farah K, et al. Implementing family-centered care in early intervention for children with hearing loss: Engaging parents with a question prompt list (QPL). Hearing Review. 2017;24(11):12-18.
References
-
Gravel JS, McCaughey CC. Family-centered audiologic assessment for infants and young children with hearing loss. Seminars in Hearing. 2004;25(4):309-317. DOI: 10.1055/s-2004-836133
-
Harrison M, Roush J. Providing information at diagnosis: Advice from parents. Volta Voices. 2004;11:6-7.
-
Moeller MP, Carr G, Seaver L, Stredler-Brown A, Holzinger D. Best practices in family-centered early intervention for children who are deaf or hard of hearing: An international consensus statement. J Deaf Stud Deaf Educ. October 2013;18(4):429-445. doi: 10.1093/deafed/ent034
-
Centers for Disease Control and Prevention (CDC). Hearing loss in children: 2014 summary of early intervention (EI) among infants identified with permanent hearing loss. Available at: https://www.cdc.gov/ncbddd/hearingloss/2014-data/2014_EI_Summary_Web_3.pdf. Available August 2016.
-
Harrison M, Page TA, Oleson J, et al. Factors affecting early services for children who are hard of hearing. Lang Speech Hear Serv Sch. January 2016;47:16-30. doi:10.1044/2015_LSHSS-14-0078
-
DesGeorges J. Working with challenging and under-involved families. In: Seewald RC & Bamford JM, eds. Proceedings from the Phonak 2010 Sound Foundations Conference. Chicago: Phonak; 2010;291-295. Available at: https://www.phonakpro.com/content/dam/phonakpro/gc_hq/en/events/2010/pediatric_audiology_conference_chicago/Pho_Chap_23_DesGeorges%20final.pdf
-
Singh G, Hickson L, English K, et al. Family-centered adult audiologic care: A Phonak position statement. Hearing Review. 2016;23(4):16.
-
Brown RF, Bylund CL, Li Y, Edgerson S, Butow P. Testing the utility of a cancer clinical trial specific Question Prompt List (QPL-CT) during oncology consultations. Patient Ed Counseling. August 2012;88(2):311-317.
-
Butow PN, Dunn SM, Tattersall MHN, Jones QJ. Patient participation in the cancer consultation: Evaluation of a question prompt sheet. Annals Oncol. March 1,1994;5(3):199-204.
-
Ahmed R, McCaffery KJ, Aslani P. Development and validation of a question prompt list for parents of children with attention-deficit/hyperactivity disorder: A Delphi study. Health Expectations. January 19, 2015;19(2):234–252. DOI: 10.1111/hex.12341
-
Lederer S, Fischer MJ, Gordon HS, Wadhwa A, Popli S, Gordon EJ. A question prompt sheet for adult patients with chronic kidney disease. BMC Nephrol. October 19, 2016;17:155. DOI: 10.1186/s12882-016-0362-z
-
Yeh JC, Cheng MJ, Chung CH, Smith TJ. Using a question prompt list as a communication aid in advanced cancer care. Journal of Oncology Practice. May 2014;10(3): e137-e141. DOI: 10.1200/JOP.2013.001295
-
Clayton J, Butow P, Tattersall M, et al. Asking questions can help: Development and preliminary evaluation of a question prompt list for palliative care patients. British Journal of Cancer. November 2003;89:2069-2077. doi:10.1038/sj.bjc.6601380
-
Sansoni J, Grootemaat P, Duncan C, Samsa P, Eagar K. A systematic literature review on Question Prompt Lists in health care (Final Report). Centre for Health Service Development, University of Wollongong;June 2014.
-
Flesch R. A new readability yardstick. J Applied Psychol. 1948;32(3):221- 233. DOI: http://dx.doi.org/10.1037/h0057532
-
National Institutes of Health (NIH). How to write easy-to-read health materials. Washington, DC: NIH/US National Library of Medicine. Available at: http://www.nlm.nih.gov/medlineplus/etr.html. Accessed September 15, 2017.
-
Weiss BD. Health Literacy: A Manual for Clinicians. Chicago: American Medical Association, American Medical Foundation;2003.
-
Bensing JM, Verhaak PFM. Communication in medical encounters. In: Kaptein A, Weinman J, eds. Health Psychology. Malden; Oxford; Victoria: British Psychological Society; Blackwell Publishing, 2004:261-287.
-
Brandes K, Linn AJ, Butow PN, Van Weert JCM. The characteristics and effectiveness of Question Prompt List interventions in oncology: A systematic review of the literature. Psycho-Oncol. 2015;24(3):245-252. doi: 10.1002/pon.3637
-
Pajevic E, English K. Teens as health care consumers: Planned transition and empowerment. Audiology Today. 2014;26(6):14-18.
-
Centers for Disease Control and Prevention (CDC). Questions you may want to ask your child’s audiologist. Washington, DC: CDC;2012. Available at: https://www.cdc.gov/ncbddd/hearingloss/freematerials/audiologist_questions_eng.pdf



