This study, which replicates earlier research on feedback cancellation (FBC) systems, uses three tests to evaluate the various aspects of hearing aid performance directly affected by the FBC: AGBF, Max-REIG, and a sound quality evaluation using Multi-Stimulus Test with Hidden Reference and Anchor (MUSHRA). It finds that significant discrepancies still exist among manufacturers in terms of AGBF and Max-REIG, and there remain trade-offs when reviewing the results of max-gain and the sound quality ratings together. However, considering all potential trade-offs, the Signia FBC can be considered a best-in-class algorithm in this multifaceted benchmark analysis.
Tech Topic | April 2018 Hearing Review
There has been much discussion over the years of hearing aid technologies which improve the signal-to-noise ratio (SNR) at the ear. Receiving considerably less attention, however, is perhaps the most significant modern advancement in hearing aid technology of all—improved feedback reduction systems.
Until recently, it was generally accepted by both hearing care professionals (HCPs) and their patients that hearing aids would “whistle” while being worn. Far from being a minor issue, these audible artifacts, due to acoustic feedback (also referred to simply as feedback), carry with them serious negative consequences.1
For example, acoustic feedback may lead to issues of loudness discomfort, sound annoyance, reduced sound quality, and even reduced speech understanding. Hearing aid wearers with feedback issues—not knowing what other options are available to them—often use the onset of feedback as a criterion for setting the instrument’s gain control. Unfortunately, this setting commonly is below the gain levels necessary for maximal speech understanding, thereby reducing the perceived benefit of amplification and likely contributing to hearing aid rejection rates.
The presence of acoustic feedback can also reinforce negative stigmas surrounding hearing aid use in the minds of non-users. Mueller et al1 describes how encountering audible feedback serves to support the largely unfounded, but prevalent, opinion among potential hearing aid users that hearing aids don’t work very well. A whistling hearing aid during the middle of a church service sends a clear message that the user just spent thousands of dollars for something that is not working. Who would want to be that person? Reducing the stigma associated with hearing aid use is an important step towards increasing acceptance of hearing aids.
Fortunately, modern feedback reduction algorithms have come a long way towards addressing feedback-related difficulties. Back in the 1990s, Mead Killion coined the term ABONSO, an acronym for “automatic brain-operated noise suppression option.” His point was that delivering effective audibility at key speech frequencies, and allowing the brain to process the signal, might be as effective as some noise reduction strategies. Many of today’s feedback reduction algorithms allow us to do just that—adding 10 dB or more of gain in an open fitting that previously was not possible.
The techniques and algorithms used in modern hearing aids to suppress acoustic feedback are reviewed by Ricketts et al.2 Most manufacturers employ some form of feedback cancellation (FBC), which uses the frequency and phase response of the feedback initialization process to model an internal feedback path. This can be accomplished using either a static or adaptive filter approach, and some systems also use frequency/phase shifting.
Given that different manufacturers use similar methods for feedback reduction, it is tempting to assume that the real-world benefits for patients using the different instruments will also be similar. This is probably not true.
There are two clinical methods to assess the quality of a given feedback reduction system using probe-mic measures with hearing aid users (for a review, see Mueller et al4). One method is to measure added gain before feedback (AGBF). Using this approach, with feedback suppression deactivated, the gain of the hearing aid (originally programmed to a prescriptive target such as NAL-NL2) is raised until feedback occurs. The real-ear aided response (REAR) is recorded. The feedback reduction algorithm is then activated and the process is repeated. The difference between the two REARs is the AGBF. The limitation of this approach is that if the output of a given product is relatively stable with feedback reduction “off,” the maximum output of the hearing aid might be reached with feedback reduction “on” before feedback occurs, preventing the assessment of true AGBF. AGBF, however, does answer the most basic question of how well the FBC prevents audible feedback for a given product. That is, it determines effectiveness of FBC with regards to gain only, providing an indication of technological leverage, which is less relevant for the practicing clinician.
A second method to assess the effectiveness of FBC systems is to simply measure the maximum real-ear insertion gain (REIG) that is available with the feedback reduction algorithm “on.” This approach is helpful from a clinical standpoint, as it provides handy product-specific guidance regarding the degree of hearing loss that can be fitted without feedback.
Ricketts et al,2 based in part on the work of Marcrum and Ricketts,3 report on their findings using this max-REIG approach for the premier hearing aid of seven leading manufacturers. The hearing aids were all mini-BTEs and were fitted with open eartips. The Max-REIG findings from Ricketts et al2 are shown in Figure 1.
The data in Figure 1 demonstrates that at least at the time of this testing (circa 2012), there was a large difference in the effectiveness in feedback reduction systems for the different manufacturers. Consider, that if an HCP were to choose HA-1 or HA-2, they would not be able to achieve desired gain in the high frequencies with an open fitting for anyone with more than a ~50 dB hearing loss, as Max REIG is only 15-25 dB. On the other hand, as shown on Figure 1, with some of the other products, it’s possible to achieve feedback-free gain of 30-35 dB, allowing for open fittings for individuals with hearing loss of 70 dB or more.
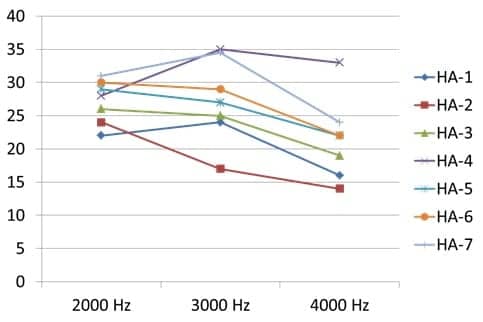
Figure 1. Mean maximum real-ear gain (n=16 ears) achieved for seven different manufacturers for open fittings (mini-BTE instruments) with feedback-reduction processing activated. Adapted from Ricketts et al.2
Using the Max-REIG approach provides an indication of how much headroom is available for the fitting, and is very relevant in clinical practice. But, like AGBF, Max-REIG does not reflect the effect of the FBC on the general sound quality of the hearing aid, an increasingly important aspect to consider. This is because overzealous FBC systems—which attempt to eliminate potential feedback as quickly as possible—often introduce distortions and artifacts which undermine the general sound quality. As hearing aid wearers are becoming younger, more technologically savvy, and demanding, these compromises in sound quality are also less acceptable. Therefore, any thorough analysis of an FBC system should also include a sound quality assessment. However, these assessments are also more difficult to conduct, because they rely on subjective measures; particular care needs to be taken to assess them in a comparative study with the lowest risk of introducing bias.
To determine if the large differences reported by Ricketts et al2 continue to exist today and to evaluate the effects of the FBC on the sound quality of the amplified signal, a comparative feedback reduction study was designed and conducted by Steven Marcrum, AuD, PhD, at the University Hospital Regensburg in Regensburg, Germany.
Method
The premier hearing aids from the top six global hearing aid manufacturers were evaluated in this study, including Signia Pure 13 BT. Three separate tests were conducted to evaluate the various aspects of hearing aid performance directly affected by the FBC:
- AGBF,
- Max-REIG, and
- A sound quality evaluation using Multi-Stimulus Test with Hidden Reference and Anchor (MUSHRA).
The hearing aids studied were Signia Pure 13 BT and the premiere mini-BTE RIC instruments from five other leading hearing aid manufacturers.
A total of 20 adults with normal hearing participated in the study. They were fitted unilaterally with each of the six hearing aids using the same gain configuration for a sloping 20 to 65 dB hearing loss.
The NAL-NL2 prescriptive formula was used as the reference, and the hearing aids were programmed for 250-6000 Hz within 2 dB of target in a 2cc coupler using a 50 dB SPL International Speech Test Signal (ISTS). The hearing aids were all programmed to an omni-directional microphone pattern with adaptive parameters deactivated (noise reduction, frequency lowering, etc) to the extent possible using the respective programming software. To account for differences in compression, an effort was made to linearize gain as much as possible. All hearing aids were fitted to the participants using soft plastic open ear-tips, as supplied and recommended by each manufacturer. The openness of each fitting was confirmed via comparison of the real-ear unaided response (REUR) to the real-ear occluded response (REOR) for each individual ear. In all cases, the REOR only deviated slightly from the REUR.
For both the AGBF and Max-REIG testing, each participant was seated upright with arms placed on a chair armrest. The point of feedback was determined by globally increasing and decreasing master gain in 1 dB steps. The presence of feedback was determined by a normal-hearing expert examiner monitoring the hearing aid sound output in the participant’s ear canal via headphones. The same listening expert performed all tests so as to minimize any individual bias between the comparisons.
In order to enhance the clinical relevance of the study outcome, the study attempted to replicate situations consistent with the patients’ real-world experiences. To that end, feedback was elicited by the researcher waving a hand several inches from the aid, by whistling, and by presenting a speech signal at 50 dB SPL. In addition, feedback was elicited by having the participant open and close his or her mouth repeatedly and by turning the head in all directions.
Once the point of feedback was determined, the output of the hearing aid was reduced by 2 dB. This setting was used for the REAR measure with the feedback reduction system turned off and on. The 2-dB below feedback value was chosen because this is typically the level where instability in output occurs before audible feedback becomes persistent. AGBF was then determined by subtracting the REAR with FBC off from REAR with FBC on. Max-REIG was calculated by subtracting each given ear’s measured REUR from the REAR observed with feedback suppression on.
The order in which hearing aids were tested was randomized across participants. Participants were also blinded to the manufacturer.
For the listening test portion of the study, a Multi-stimulus test with Hidden Reference and Anchor (MUSHRA) method was employed to compare the various feedback reduction systems on sound quality. The test signals were both speech (male and female German talkers) and music (female opera singer with orchestral background) stimuli. A full-band reference and 1 kHz low-pass anchor were hidden within the hearing aid recorded signals. Test signals presented at 50 dB SPL were recorded for each hearing aid mounted on KEMAR. In the same manner as described earlier, each hearing aid gain was adjusted within KEMAR’s ear to 2 dB below the feedback point. This was done to provide an estimate of each hearing aid’s sound quality when the given aid was operating close to its limit.
Because different products reached feedback at different outputs, this also meant that the recordings were performed at different gain levels. To account for these differences in loudness, therefore, RMS levels were equalized for each hearing aid post-recording. A group of 30 normal-hearing participants were asked to listen to these recordings under HDA 200 headphones bilaterally, and rate the sound quality of each sample with a visual-analog scale of 0 to 100 with scale anchors. Each subject was presented with 8 stimuli to rate (6 hearing aid recordings, 1 reference, and 1 anchor). This was conducted separately for both the speech and music sound samples. The order of test signals was randomized for each participant. All participants correctly identified the full-band reference.
Results
Measurement of additional gain before feedback (AGBF) showed that, except Brand B, the other five hearing aids were able to provide 9 dB or more of additional gain around the feedback-critical area of 2 to 4 kHz (Figure 2). The highest AGBF was for Brand E at 16.3 dB, and with an AGBF of 14.7 dB, Signia was not significantly lower.
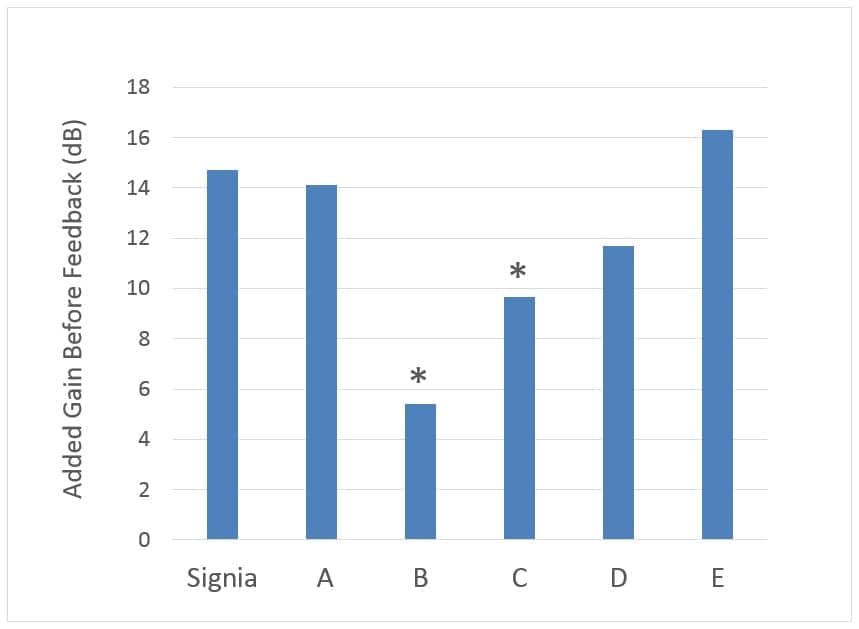
Figure 2. Average AGBF for six premiere hearing aid brands. The AGBF represents the difference between the real-ear aided response just below feedback for feedback suppression “On” vs “Off.” Results significantly different from Signia are indicated with an asterisk (*).
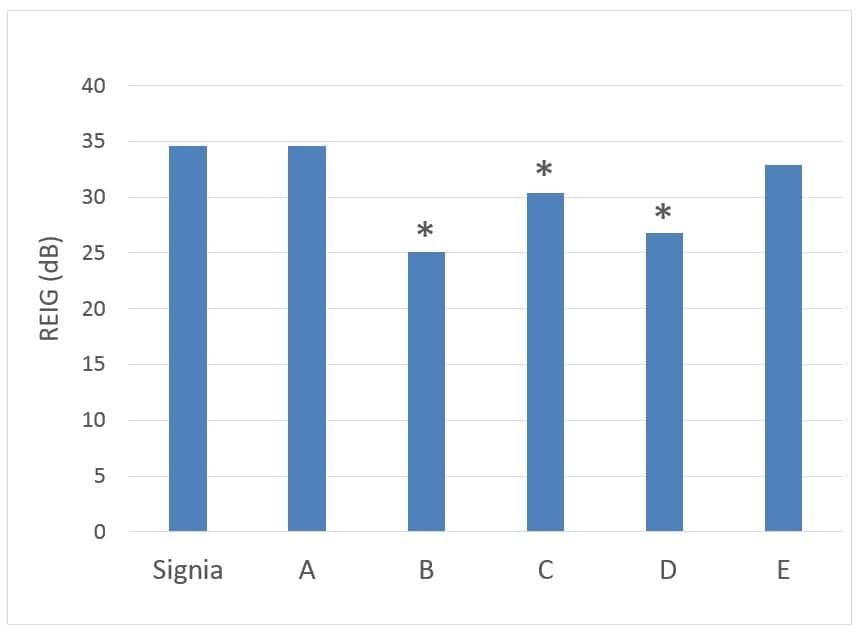
Figure 3. Average Max-REIG at 2 to 4 kHz for six premier hearing aid brands. Max-REIG was calculated by subtracting the REUR from the REAR for each individual ear with feedback suppression on. Results significantly different from Signia are indicated with an asterisk (*).
Similar results were obtained with the measurement of Max-REIG from 2 to 4 kHz (Figure 3). The three top performers were Signia, Brand A, and Brand E, providing the highest REIGs before feedback of 35 dB, 35 dB, and 33 dB, respectively. Brand B again showed the poorest performance, providing the least insertion gain at 25 dB.
The findings for the sound quality ratings are shown in Figure 4. Since the overall pattern was similar for both the music and speech stimuli, the results shown are the average of the two signals. Given that overzealous FBC systems can have an adverse effect on sound quality, it is perhaps not surprising that the product with the poorest performance for both the AGBF and the Max-REIG measures, Brand B, had the highest rating for sound quality. The ratings for Brand A were rated to have the worst sound quality. The other four hearing aids, including Signia, were rated similarly, and were not significantly different from each other.
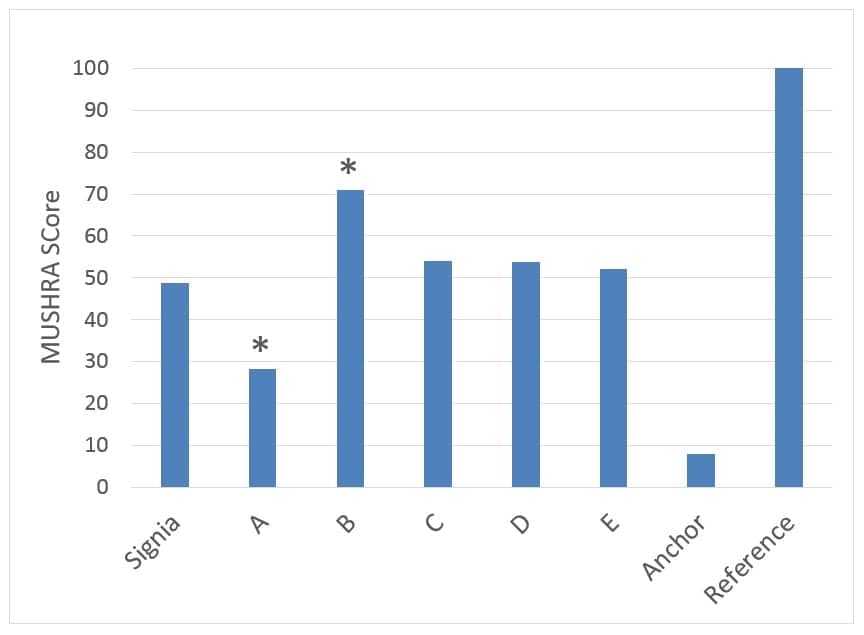
Figure 4. Sound quality results, averaged for the speech and music stimuli, for the six premiere hearing aids with output set “just-below-feedback,” using the MUSHRA approach. Results significantly different from Signia are indicated with an asterisk (*).
Discussion & Conclusion
As mentioned, portions of this study were a replication of the earlier work of Marcrum and Ricketts,3 and those reported by Ricketts et al,2 as shown in Figure 1. Comparing the results from this study to that of Ricketts et al,2 it is encouraging to see that all six of the hearing aid manufacturers now offer FBCs which provide at least 25 dB of Max-REIG for open fittings for the important higher frequencies. Note that the differences in Max-REIG among manufacturers shown in Figure 1 are as large as 17-18 dB; the differences in this study are around 10 dB. The top products do not appear to have changed significantly (perhaps the limits of the technology), but the bottom products have improved.
Nevertheless, significant discrepancies still exist among manufacturers in terms of AGBF and Max-REIG. Providing an extra 10 dB of gain can have a significant effect for many hearing aid users in need of audibility of high-frequency speech signals. For example, Valente et al5 recently reported that when gain in the high frequencies falls 10 dB or so below NAL-NL2 values, speech recognition for soft speech is reduced by 15%, and real-world benefit is significantly reduced based on the Abbreviated Profile of Hearing Aid Benefit (APHAB).
When reviewing the results of max-gain and the sound quality ratings together, it is clear that there is somewhat of a trade-off between these two factors. Hearing aid FBCs which provide more stable gain and a wider fitting range tend to be rated slightly less favorably for sound quality under the given approach, which was close to the feedback limit. The one hearing aid with significantly less-effective FBC (ie, Brand B) is perceived to offer better sound quality.
As shown, the Signia is among the manufacturers to provide most effective FBC, as shown by AGBF, and it provides the highest insertion gain before feedback, as shown by average Max-REIG data. Yet, it is still rated comparably to other premiere hearing aids on the market in terms of sound quality. Consider, that the sound quality ratings shown here were from individuals with normal hearing—the small advantage for Brand B might not be present for individuals with hearing loss and cochlear damage.
Overall, the quality of a product’s feedback cancellation technology is one of the most important considerations when selecting hearing aids for a given patient—especially when open fittings are employed. Considering all potential trade-offs, the Signia FBC can be considered a best-in-class algorithm in this multifaceted benchmark analysis.
Acknowledgements
We would like to acknowledge Dr Marcrum for his helpful comments on previous versions of this manuscript.
References
-
Mueller HG, Ricketts TA, Bentler R. Modern Hearing Aids: Pre-Fitting Testing and Selection Considerations. San Diego: Plural Publishing;2014.
-
Ricketts TA, Bentler R, Mueller HG. Essentials of Modern Hearing Aids: Selection, Fitting, and Verification. San Diego: Plural Publishing;2018.
-
Marcrum S, Ricketts TA. Assessment of modern feedback reduction systems. Paper presented at: American Auditory Society AAS Annual Meeting; March, 2011; Scottsdale, AZ
-
Mueller HG, Ricketts TA, Bentler R. Speech Mapping and Probe Microphone Measurements. San Diego: Plural Publishing;2017
-
Valente M, Oeding K, Brockmeyer A, Smith S, Kallogjeri D. Differences in word and phoneme recognition in quiet, sentence recognition in noise, and subjective outcomes between manufacturer first-fit and hearing aids programmed to NAL-NL2 using real-ear measures. JAAA. 2017.
Correspondence can be addressed to HR or Dr Herbig at: [email protected]
Citation for this article: Herbig R, Lueken C. A comparison of feedback cancellation systems in premier hearing aids. Hearing Review. 2018;25(4):20-23.



Hello
Can you tell me the order of the HA brands from the best one to the worst one as a result of the FBC systems and name these brands ?
you need an independent such as Dr Ruth Bentler to evaluate feedback systems in the different company’s I don’t have much faith in any company’s research on their own products
Hi Robert. Thanks for your comment. As stated in the article, the research indeed was conducted by an independent researcher; Steven Marcrum, AuD, PhD, at the University Hospital Regensburg in Regensburg, Germany. Dr. Marcrum is a respected researcher and has several peer-reviewed publications related to hearing aid processing. Moreover, Dr. Marcrum had completed a similar independent study several years ago while working with Todd Ricketts at Vanderbilt University.
It would be interesting to see this study performed without the funding and bias from one company. An independent study revealed what the other manufacturers are would be preferable.
Hi Kevin, thanks for your comment. The research was conducted by an independent researcher; Steven Marcrum, AuD, PhD. Dr. Marcrum is a respected researcher and has several peer-reviewed publications related to hearing aid processing. We have no reason to question Dr. Marcrum’s integrity.
Hi dear colleauge
Can you tell me, which brand used in these article?
Hi Vahid, thanks for your comment. As stated in the article, the hearing aid were from the six leading brands globally: Signia, Oticon, Phonak, ReSound, Starkey, and Widex.