A Moisture Resistant Switch for Improving the Robustness of BTEs
A technical review of a new moisture-resistant sealed switch for hearing aids.
Read More
A technical review of a new moisture-resistant sealed switch for hearing aids.
Read More
A review of the latest in impression material technology and related accessories.
Read More.gif)
Current thinking on managing a low frequency hearing loss supports the use of broadband, multichannel WDRC hearing aids. In this way, both the low frequency and mid-to-high frequency cochlear fibers can be stimulated. This article examines the issues and decisions involved when fitting reverse-slope losses.
Read More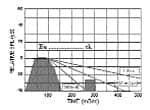
In some cases, processing properties of AGC hearing aids may be contributing to the difficulties encountered by hearing aid wearers, says this technical report. A look at this premise and the development of an alternative processing approach to reduce reverberation is offered.
Read More
A patient’s stimulated auditory response should never exceed their loudness discomfort level (LDL) at any frequency, or there is a good chance they will reject the fitting. Here are the basics on testing for loudness discomfort.
Read MoreHearing aid selection is a critical step in the amplification process. With today’s vast array of choices in hearing instrument technology, where do you start? Part 2 of this three-part series examines hearing aid selection by measurement, matrices, and prescriptive formulae.
Read More