Annual HR Literature Review
A review of the latest in manufacturer literature and promotional/marketing materials.
Read More
A review of the latest in manufacturer literature and promotional/marketing materials.
Read MoreAmplification and bone conduction options for those with idiopathic sudden sensorineural hearing loss (ISSNHL), and why counseling is the key to success.
Read More
One of the keys to assisting the SSNHL patient is to understand the diagnostic and treatment pathways for the patient. This article looks at the evaluation, management, natural history, and rehabilitation of the SSNHL patient.
Read More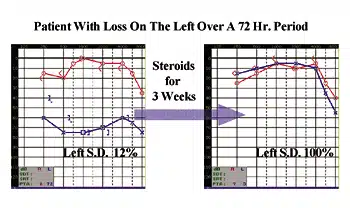
Recent research at the Massachusetts Eye and Ear Infirmary and Harvard Medical School has significant implications for the use of steroid therapy with SSNHL patients.
Read More
Sudden hearing loss is a complex disorder with significant uncertainties and highly variable outcomes. A team approach is vital in efforts to achieve optimal outcomes.
Read More
Sudden hearing loss is a common medical emergency, with 5 to 20 individuals per 100,000 population per year experiencing SSNHL. Two otologists from the House Ear Institute explain the causes and treatment strategies for sudden hearing loss.
Read MoreAn introduction to the topic of sudden sensorineural hearing loss (SSNHL), and a look at the issues and articles discussed in this special edition of The Hearing Review.
Read More