A New Tool for Fighting Feedback in BTEs
A method for using stents to eliminate feedback during problem fittings.
Read More
A method for using stents to eliminate feedback during problem fittings.
Read MoreA new client education tool is designed to de-emphasize specific products and de-mystify the information on a wide range of technologies, styles, and price ranges for the consumer.
Read More
A sneak-peek at the products, services, and events being offered at the International Hearing Society’s (IHS) annual convention in Orlando, August 25-29.
Read MoreThe new HIPAA Security Rules, which start April 21, 2005, will require hearing care professionals to modify their policies with regard to their patients’ electronic protected health information.
Read More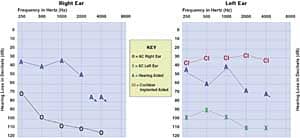
A look at the rationale behind directional hearing aids that have the ability to automatically switch between directional and omni-directional modes, as well as fitting tips that ensure proper microphone orientation, venting of the aid, demonstration of directional benefit, and counseling.
Read More
Part 1 of a 2-part article that provides information on fitting a hearing aid to the opposite ear of a cochlear implant. Part 1 provides information on attaining the proper hearing aid gain, frequency response, and loudness balance relative to the cochlear implant.
Read More