Hearing Dogs: Farewell to Dana the Wonder Dog
Hearing dogs are valuable in many different ways.
Read More
Hearing dogs are valuable in many different ways.
Read More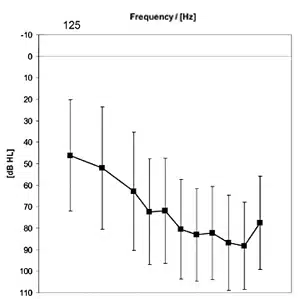
A field trial involving the Phonak Smartlink FM transmitter
Read More
A sneak-peek at the new products, services, and events being offered at the 17th Annual American Academy of Audiology (AAA) convention held in Washington DC on March 30-April 2.
Read More
Although vent diameter decreases the directivity index of a directional hearing aid, a significant directional and noise reduction benefit is still available even with an open fitting. This study suggests that open fittings appear to be most beneficial (or least compromising) for people with milder hearing losses, or precipitous loss with normal low-frequency hearing where SNR loss may be milder.
Read More
Part four of a four-part series on staff management for private practice entrepreneurs. This article discusses how to motivate staff members–and create conditions for them to motivate themselves.
Read More
In a study of 67 subjects, 51% experienced changes of 10% or more in ear canal volume (ie, volume increase or decrease in at least one ear) when opening their jaw. This suggests that, in fittings involving physical discomfort or shell-related problems, the problem may be the ear and not the impression.
Read More