A New High-Performance Fully Transparent Hearing Instrument
Speech clarity, sound quality, fitting accuracy, and open-ear comfort are the design functions of a newly introduced hearing instrument platform and product line.
Read More
Speech clarity, sound quality, fitting accuracy, and open-ear comfort are the design functions of a newly introduced hearing instrument platform and product line.
Read More
A new hearing instrument in which electronic information is shared between two hearing aids in a binaural fitting has now also employed an open-fitting solution.
Read More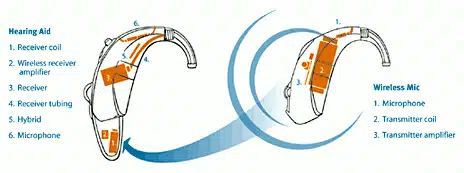
One clinician’s experiences using WiFi technology that beams signals to the hearing aid in a CROS fitting (ie, no cables), and the acceptance of the technology by her patients.
Read More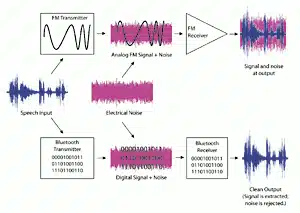
An ear-level Bluetooth device has been introduced that allows hands-free operation of a cell phone along with hearing aid compatibility. The authors believe this represents only the beginnings for this type of technology in hearing aid applications.
Read MoreAre professional ethics in the “eyes of the beholder”? Yes, the consumers’ eye. A perspective on ethics in private practice and how philosophy must dictate practice.
Read More
The keys to a successful practice include good office presentation, adopting a patient-driven model of care, effectively overcoming objections, and measuring the overall patient benefit.
Read More
How do you know that a hearing instrument works to specification? The ANSI test remains a useful tool for verifying the operational status of a device.
Read More