How Hearing Aid Access May Be Improved Using Ultrawideband Technology
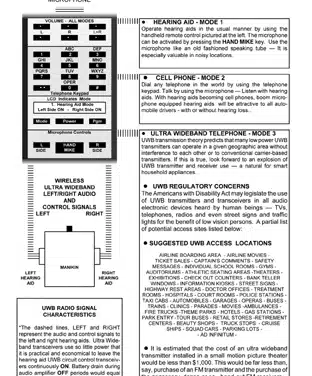
A fun look into the crystal ball for the ultimate wireless hearing system With the advent of ultrawideband (UWB) radio, the author envisions that many hearing aids will be equipped with UWB transmitters and receivers that will be fully controlled by a wristwatch-like keypad. This, in turn, might also be equipped with an UWB transmitter and receiver for connection to your cellphone or hard-wired telephone.
Read More