
Each year, approximately 9 million people worldwide search for a solution to hearing loss. Depending on the degree and nature of their hearing loss, one of three treatments may be suitable: conventional air-conduction hearing aids, cochlear and middle-ear implants, and bone-conduction hearing devices, including Baha® (an osseointegrated hearing device). Although each of these treatments seeks to overcome the difficulties caused by hearing loss, the differences among these approaches provide specific advantages for different populations.
Treatments for Hearing Loss
Conventional hearing aids, the most common solution, aim to overcome the degree of conductive or sensorineural hearing loss by amplifying the incoming signal and sending the amplified sound via air conduction through to the cochlea. Candidates for conventional air-conduction hearing aids include those with mild to severe sensorineural hearing loss, conductive, and/or mixed hearing loss.
Cochlear implants are suitable for individuals with a severe or profound hearing loss, where the extent of destruction to the cochlea’s hair cells is so great that hearing aids are unable to provide benefit. In cochlear implants, sound is picked up and processed by the sound processor and the cochlea is electrically stimulated, thus restoring the sensation of hearing. This process compensates for the destruction of the hair cells by routing the signal directly to the auditory nerve.
|
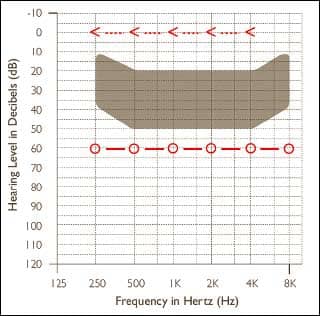
| FIGURE 1. Audiogram representing an idealized total conductive hearing loss. Arrows indicate bone-conduction thresholds and circles indicate air-conduction thresholds. Sounds useful for speech are represented by the shaded area. |
Baha provides an optimal amplification choice for those with conductive, mixed, or single-sided sensorineural deafness through the use of direct bone conduction. The Baha consists of three parts, the ossiointegrated implant, the sound processor, and the abutment that connects the two. The sound processor is connected directly to the skull through an osseointegrated titanium implant in the temporal bone. Sound vibrations are thereby passed through the titanium implant and vibrate the temporal bone that houses the cochlea, thereby providing the sensation of hearing. Bone conduction thereby overcomes conductive hearing loss by innervating the cochlea directly. It can also compensate for a degree of sensorineural hearing loss in a mixed hearing loss with increased amplification. Additionally, Baha provides a solution for individuals with single-sided sensorineural deafness, as the skull can efficiently conduct the sound from one side of the head to the opposite cochlea.
Importantly, while there are a number of implantable technologies for hearing loss (eg, middle-ear implants), Baha remains the only technology that the patient can thoroughly evaluate before surgery. Through the use of a softband or test rod, the patient is able to evaluate in advance the potential benefits of Baha.
Conductive Hearing Loss
Baha is a frequent choice for permanent conductive hearing loss. This is, in part, because conductive hearing loss is often concomitant with various outer- and middle-ear abnormalities (eg, atresia) or middle-ear pathologies (eg, continuously draining ear) that preclude hearing aid use.

|
| FIGURE 2. Aided Baha thresholds indicating the sound-field thresholds that may be expected from a Baha for patients with a conductive hearing impairment.1 |
Figure 1 gives an indication of the sound a patient with this type of hearing loss is missing. Much of the speech signal is largely inaudible. With Baha, the conductive element of the hearing loss is bypassed by sending sound vibrations directly from the sound processor, through the skull, and to the cochlea. As can be seen in Figure 2, postoperative aided responses when wearing the Baha are excellent, and the patient is able to obtain near-normal auditory thresholds.1
Even without medical indications, the Baha provides significant benefits over conventional hearing aids due to large gain requirements. Because of the abnormal growth of loudness caused by sensorineural hearing loss, most hearing aid rationales prescribe approximately 50% gain of the degree of hearing loss. For example, for a sensorineural hearing loss of 60 dBHL, the hearing aid would prescribe approximately 30 dB of gain.
For conductive hearing loss, however, loudness growth is essentially normal. Therefore, one would consider providing 100% compensation for the degree of conductive hearing impairment. Counterintuitively, most published prescriptive formulae recommend only 75% compensation for the conductive element.2,3 Interestingly, this decision has been based on the technical limitations of the hearing aid rather than the needs of the patient. A number of technical limitations arise when attempting to fit hearing aids to larger conductive loss. These include insufficient gain, saturation, feedback, and also the necessity of a tight-fitting earmold. The insufficient power of most hearing aids compromises the hearing performance of the patient with conductive hearing loss.
Baha provides an optimum solution for patients with conductive hearing loss because the treatment avoids difficulties associated with middle-ear pathology and the limitations of hearing aids.

|
| FIGURE 3. Audiogram showing an example of a significant mixed hearing loss. Circles represent air-conduction thresholds and arrows represent bone-conduction thresholds. Sounds useful for speech are represented by the shaded area. |
Mixed Hearing Loss
For patients with a mixed hearing loss (Figure 3), Baha provides a two-fold solution. First, it closes the air-bone gap by bypassing the conductive element. Second, it compensates for the remaining degree of sensorineural hearing loss. To achieve this, an additional amplification force is required to compensate for the degree of sensorineural deafness. As shown in Figure 4, the resultant aided free-field thresholds are extremely good with the device, providing excellent compensation for the sensorineural element of the mixed hearing loss.
New transducer increases power. A new device, the Baha Intenso™, compensates for up to 55 dBHL of sensorineural hearing loss (current CE indication; expanded indication awaiting approval from FDA). As observed in Figure 5, Intenso produces 10-15 dB more gain for the patient through the use of a more powerful transducer and an active feedback cancellation system.
When deciding on treatment options, it is important to remember that the overall amplification required for people with a mixed loss is less with a Baha than that required for a hearing aid. Put simply, the device bypasses the conductive element of the hearing loss and addresses the sensorineural component directly. This provides a more efficient and comfortable method of sound transmission to the cochlea.

|
| FIGURE 4. Example of the aided sound-field thresholds following the fitting of a Baha for a patient with mixed hearing loss. |
Conversely, the air conduction hearing aid must address both the conductive and sensorineural elements. While hearing aids are good at compensating for sensorineural hearing loss, compensation for the conductive element rapidly increases the required gain and maximum power output. These requirements indicate that conventional air conduction hearing aids may have insufficient overall power and that saturation from loud inputs will occur more readily.
Air-bone gap exceeding 30 dB indicates consideration of device. Approximately 18% of patients with a severe or profound hearing loss have a significant mixed component to their loss. Given the limitations of conventional hearing aids, and the capability of Baha, numerous studies4-9 recommend that, when the conductive component of the mixed hearing loss becomes greater than 30 dB, Baha should be the amplification method of choice. For patients in these studies, Baha performed significantly better than conventional air-conduction hearing aids in terms of aided thresholds, speech perception measurements, and subjective reports. Improvements in speech understanding in noise afforded by greater high-frequency audibility in Baha were also reported.8
Therefore, for patients with air-bone gaps greater than 30 dB, Baha should be evaluated as a potential amplification option due to numerous reports indicating significant benefit when compared to traditional air-conduction amplification.

|
| FIGURE 5. Increase in available gain with Baha Intenso that is available with the implementation of an active feedback cancellation system. |
Single-Sided Deafness
Single-sided sensorineural deafness (SSD™) poses significant communication difficulties for the patient. Primarily, this difficulty is due to the inability to accurately localize where sound is coming from. In addition, speech-understanding difficulties arise in situations where the noise is directed toward the good ear and the talker is near the deaf ear. In many situations (eg, driving a car), the patient is unable to compensate for this difficulty by changing head position. Recently, a number of studies have demonstrated the efficacy of Baha for people with SSD.8,10-14
For patients with SSD, the Baha is worn on the deaf side, and it transfers the signal directly across the skull via bone conduction, thus eliminating the head shadow effect described above. In this way, sounds are efficiently transferred across the skull from the deaf side to the good ear via bone conduction.
For many patients, the sound will seamlessly transfer from one side to the other via bone conduction. For a small number of patients, additional amplification force may be required to overcome an increased interaural attenuation to provide sufficient loudness in the good ear. For these patients with an increased head transfer function, a more powerful device, such as the Intenso, is recommended.
SSD with some hearing loss in good ear. An expanding area of research for Baha is for patients who have a single-sided sensorineural deafness and some degree of hearing loss in the good ear. It may be for these patients that the unilateral total hearing loss increases the difficulties experienced from a mild hearing loss, and that a Baha becomes even more relevant.

|
| FIGURE 6. Improved aided thresholds in patients with a profound loss in one ear and a mild hearing loss in the contralateral ear. For all conditions, speech comes from the front and noise comes from the good side (red), deaf side (blue), or front (black). |
A recent study15 examined the efficacy of Baha Intenso for patients with a mild hearing loss in the hearing ear (Figure 6). The authors found that the additional amplification provided by the device effectively normalized performance. Before bone-anchored devices, the patient was at a significant disadvantage when speech was spoken from the deaf side. For this population, the Baha improves performance so that the patient experiences a more natural overall sound picture.
A number of studies have also compared the performance of Baha versus the more traditional solution of Contralateral Routing of Signal (CROS) hearing aids11,13 (ie, one hearing aid with two microphone attachments). These studies reported that speech understanding and subjective reports were significantly better with the Baha than with CROS-based solutions. Therefore, for patients with single-sided deafness, the bone-anchored device should be considered the treatment of choice.
Conclusions
Baha provides an additional treatment of choice that complements conventional hearing aids and cochlear implants. Osseointegration provides options for patients with conductive, mixed, or single sided sensorineural hearing losses. Many of these patients are either a challenge to fit with conventional air-conduction amplification (and often labeled “special populations”) or require ungainly and difficult solutions, such as CROS hearing aids.
-

- Maurice H. Miller, PhD, addressed the topic of sudden hearing loss and single-sided deafness in the special December 2003 edition of HR available in the online archives.

Due to the properties of bone conduction, Baha bypasses the conductive element of conductive and mixed hearing losses, resulting in a reduction in the amount of amplification required when compared to traditional air-conduction aids—devices that must overcome the conductive component. Similarly, due to the ease with which bone-conducted sounds transfer across the skull, the device offers a relatively simple solution for people with single-sided sensorineural deafness. While there are a number of implantable technologies available (eg, middle-ear implants), Baha remains the only one that the patient can thoroughly evaluate, via softband or test rod, before surgery.
The recent addition of the Baha Intenso, which compensates for up to 55 dBHL of sensorineural hearing loss (current CE indication; expanded indication awaiting approval from FDA), means that a larger population of individuals can benefit from Baha. Together with the advanced signal processing of Divino and the superpower performance of Cordelle, Intenso complements the portfolio of these devices by offering a discreet yet powerful head-worn solution.
Mark C. Flynn, PhD, is director of research and applications in the Cochlear Bone Anchored Solutions Group of Cochlear Corporation, Gothenburg, Sweden. Correspondence can be addressed to HR or Mark Flynn at .
References
- Tjellström A, Håkansson B, Granström G. Bone-anchored hearing aids: current status in adults and children. Otolaryngol Clin North Am. 2001;34(2):337-64.
- Scollie S, Seewald R, Cornelisse L, et al. The desired sensation level multistage input/output algorithm. Trends Amplif. 2005;9(4):1-39.
- Dillon H. Hearing Aids. New York: Thieme; 2001.
- Hol MK, Snik AF, Mylanus EA, Cremers CW. Long-term results of bone-anchored hearing aid recipients who had previously used air-conduction hearing aids. Arch Otolaryng Head Neck Surg. 2005;131(4):321-5.
- McDermott AL, Dutt SN, Reid AP, Proops DW. An intra-individual comparison of the previous conventional hearing aid with the bone-anchored hearing aid: the Nijmegen group questionnaire. J Laryngol Otol. 2002(28):15-9.
- Mylanus EA, Snik AF, Cremers CW. Patients’ opinions of bone-anchored vs conventional hearing aids. Arch Otolaryng Head Neck Surg. 1995;121(4):421-5.
- Mylanus EA, van der Pouw KC, Snik AF, Cremers CW. Intraindividual comparison of the bone-anchored hearing aid and air-conduction hearing aids. Arch Otolaryngol Head Neck Surg. 1998;124(3):271-6.
- Snik AF, Mylanus EA, Proops DW, et al. Consensus statements on the BAHA system: where do we stand at present? Ann Otol Rhinol Laryngol. 2005;195:2-12.
- Lustig LR, Arts HA, Brackmann DE, et al. Hearing rehabilitation using the BAHA bone-anchored hearing aid: results in 40 patients. Otol Neurotol. 2001;22(3):328-34.
- Hol MK, Bosman AJ, Snik AF, Mylanus EA, Cremers CW. Bone-anchored hearing aids in unilateral inner ear deafness: an evaluation of audiometric and patient outcome measurements. Otol Neurotol. 2005;26(5):999-1006.
- Wazen JJ, Spitzer JB, Ghossaini SN, et al. Transcranial contralateral cochlear stimulation in unilateral deafness. Otolaryngol Head Neck Surg. 2003;129(3):248-54.
- Hol MK, Bosman AJ, Snik AF, Mylanus EA, Cremers CW. Bone-anchored hearing aid in unilateral inner ear deafness: a study of 20 patients. Audiol Neurootol. 2004;9(5):274-81.
- Lin LM, Bowditch S, Anderson MJ, May B, Cox KM, Niparko JK. Amplification in the rehabilitation of unilateral deafness: speech in noise and directional hearing effects with bone-anchored hearing and contralateral routing of signal amplification. Otol Neurotol. 2006;27(2):172-82.
- Wazen JJ, Spitzer J, Ghossaini SN, Kacker A, Zschommler A. Results of the bone-anchored hearing aid in unilateral hearing loss. Laryngoscope. 2001;111(6):955-8.
- Vermiglio AJC, Soli S. Power BAHA Study. Los Angeles: House Ear Institute; May 20, 2007.


