
The Earlens Light-Driven Hearing Aid is designed to provide patients and clinicians with an amplification option that produces superior sound quality and extended bandwidth relative to traditional acoustic hearing aids. Here are answers to the top 10 commonly asked questions about the device.
Tech Topic | February 2018 Hearing Review
A new type of hearing aid has recently entered the market. Developed by Earlens, this system uses light instead of sound to transmit energy to the ear of the user. Due to the unfamiliar mechanism of action, there are some common misconceptions about this device and the potential benefits it offers. This article answers 10 commonly asked questions about why this device was developed, how it works, and who would be a good candidate for this new technology.
1) Why in the world would you need a Light-Driven Hearing Aid?
Earlens Corporation was founded with the goal of creating a hearing aid capable of providing significantly improved sound quality over conventional air conduction hearing aids. Using a new mechanism of action, the Earlens Hearing Aid overcomes the physical limitations of introducing amplified acoustic sound into the ear canal. This has allowed for a greatly expanded audible bandwidth of amplification, even when the ear canal is widely vented. Research on bandwidth has shown the potential for superior and more natural sound quality, as well as better speech understanding in complex environments.1-5
2) What is a Light-Driven Hearing Aid?
The FDA cleared a new type of hearing aid in 2015: a contact hearing aid.6 This novel technology bridges the gulf between an air conduction hearing aid (which uses an acoustic receiver to amplify the sound that vibrates the eardrum) and a middle ear implant (which vibrates the middle ear ossicles with a surgically implanted transducer).
A contact hearing aid works by non-invasively and non-acoustically vibrating the eardrum directly, which leads to the efficient delivery of wide bandwidth amplification to the ear. The Earlens Light-Driven Hearing Aid uses a small laser light to send the signal to the component that contacts the eardrum (Figure 1).
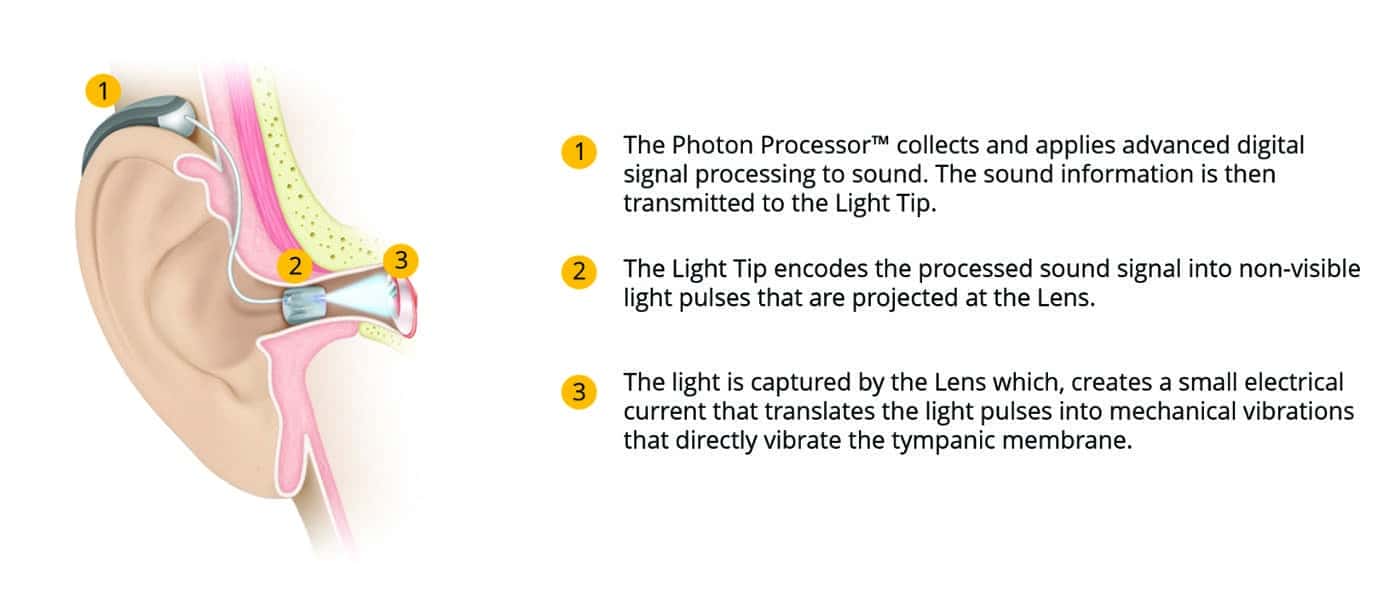
Figure 1. Schematic of the Earlens Light-Driven Hearing Aid.
The system offers individuals with mild-to-severe sensorineural hearing loss a greater bandwidth than traditional acoustic hearing aids but without the cost and surgical implications of a middle ear implant.
3) How does the Earlens Hearing Aid work?
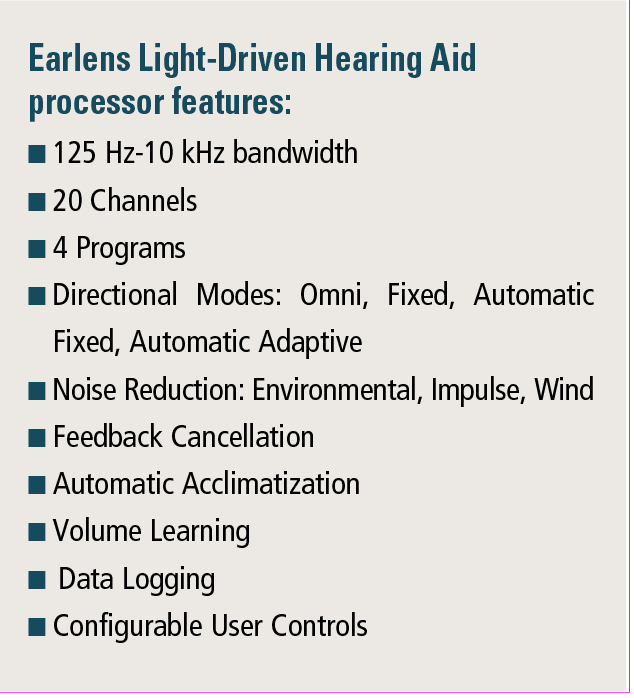
The sound processing, programming, and gain prescription philosophies of the Earlens Hearing Aid are very similar to the approach used in acoustic hearing aids. In both types of hearing aids, a digital multi-channel sound processor analyzes incoming sound and applies appropriate gain and compression for the user’s hearing loss and preference before transmitting the signal to the ear.
The two technologies diverge in the method of signal transmission. The acoustic hearing aid uses an acoustic receiver to create sound pressure to move the eardrum.
In the case of the Earlens Hearing Aid, the signal leaving the custom earmold (or “Light Tip”) is created by a very small infrared laser (Figure 1). The laser light pulses transmit power and data information to activate the customized “Lens,” the component that resides in direct contact with the umbo of the eardrum. A photodetector on the Lens converts the signal into current which, in turn, drives the motor on the Lens. A small contact platform between the Lens and the umbo enables the motor to transmit a precise vibration of the umbo with a magnitude similar to that which would be induced by air conducted sound pressure.
At this point, the technologies converge again, as the motion of the umbo in both types of technologies is passed through the ossicles, into the cochlea, and perceived as sound. While the Earlens Hearing Aid can match the output of an acoustic device in the mid-frequency regions, the unique mechanism of action allows the Earlens Hearing Aid to provide substantial output across the frequency range 125 Hz to 10 kHz while maintaining a widely vented fitting.
4) How is the Earlens Hearing Aid different from a traditional acoustic hearing aid?
While each successive generation of hearing aids has been a significant leap forward in terms of size and functionality, even the most advanced acoustic hearing aids are limited in their ability to provide audibility for speech level inputs for many patients when vented.7 This is particularly true in the high and low frequencies, due to the limitations imposed by acoustic impedance differences between the outer and middle ear, as well as gain limitations imposed by acoustic feedback. The result, in the opinion of many hearing aid users, is a listening experience characterized by artificial sound quality which fails to meet expectations.
While many hearing devices are capable of detecting and processing sound up to 9 kHz or higher, few produce audibility in those higher frequencies, and fewer still have a sufficiently occluded fitting to improve audibility in the low frequencies. In the March 2017 Hearing Review, Struck and Prusick7 illustrated the real-world effective bandwidth limitations of acoustic receivers in vented hearing aids for both low and high frequencies. Limitations in low frequencies are often due to patient preference for a more open fitting resulting in acoustic leakage from the ear canal. High-frequency limitations are due to receiver output limits and gain limitations imposed by the likelihood of encountering feedback with the substantial gain required to achieve audibility.
The Earlens Hearing Aid, with a widely vented fitting, has demonstrated gain and output well beyond what is currently possible with a vented acoustic hearing aid, achieving the necessary insertion gains to meet the Cambridge Fitting Formula (CAM2) prescriptive targets across the full frequency range from 125 Hz up to 10 kHz, with peak stable gains of up to 70 dB even at 8 and 10 kHz.8 This dramatic increase in audible bandwidth is possible for two reasons: first, the direct-drive mechanism of action is very efficient, and second, due to the lack of an acoustic output, the risk of feedback is greatly decreased.
The direct-drive mechanism also allows for substantial low-frequency output without an occlusive acoustic seal in the ear canal. This has several benefits, including:
1) The ability to provide appropriate gain for those with low-frequency loss who prefer venting to avoid occlusion;
2) Delivering substantial low-frequency output in a streaming program, even for those with normal low-frequency hearing, as this markedly improves the sound quality of streamed audio, and
3) The potential ability to improve speech-in-noise performance with signal processing improvements (eg, directional processing) with a widely vented fitting.
5) Who would benefit from a non-acoustic option in the mild-to-severe sensorineural loss population?
The fitting range of the Earlens Hearing Aid (Figure 2) is applicable to the majority of patients with hearing loss. It specifically targets sensorineural hearing losses ranging in severity from mild to severe. There are, however, medical requirements specific to the Earlens that may preclude patient candidacy. These requirements include a normal eardrum and middle ear, and sufficient physical size of the ear canal to accommodate the Lens. A significant conductive component is a contraindication for use, as energy transfer across the middle ear system is impaired in this case. The audiologist and ENT partner collaborate to determine patient suitability for the Earlens.
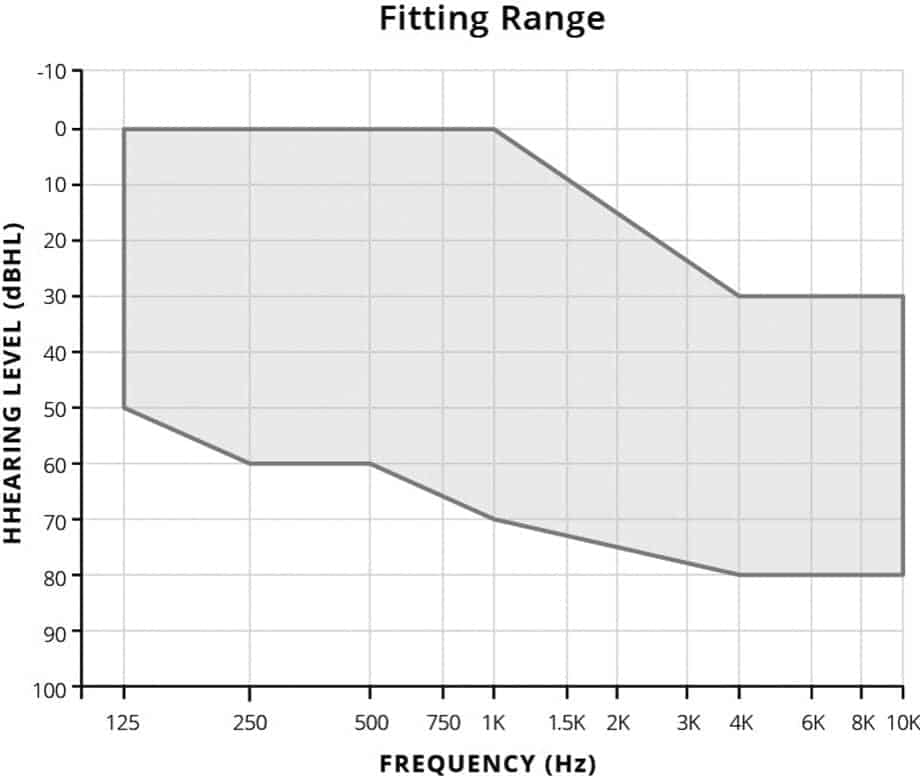
Figure 2. Earlens fitting range.
The ideal patients for the Earlens Hearing Aid are those who are seeking or are appreciative of sound quality—especially those with aidable hearing in low- and/or high-frequency regions that cannot be adequately addressed with an acoustic hearing aid, when vented, to accommodate patient preference. The Earlens device typically produces increased functional audibility compared to an as-fit hearing aid, and has the capability of delivering substantially greater gain and audibility starting at 4 kHz and continuing up through 10 kHz.9
In addition, a widely-vented (open) fitting is indicated for the entire fitting range. This makes the Earlens device particularly appropriate for patients who love to stream audio or require low-frequency amplification but dislike occlusion, as low-frequency output is not constrained by earmold venting.2

6) How is the Earlens Hearing Aid dispensed?
The Earlens Hearing Aid is dispensed and maintained through an audiologist-ENT physician partnership. This partnership provides the highest standard of care for the patient.
Following identification of audiologic and lifestyle candidacy, the patient is evaluated for medical and ear canal candidacy. Once candidacy is established, the ENT cleans the ear and uses specialized impression material and techniques to take a full-canal impression, which includes the surface of the eardrum (Figure 3a-b). At Earlens, a digital scan of this impression is used to create a three-dimensional model of the entire ear canal in order to custom design the Light Tip and Lens, as well as align the Light Tip output to the Lens photodetector (Figure 3c). At the fitting visit, scheduled approximately two weeks post-impression, the physician inserts and fits the custom Lens into the proper position to achieve precise contact with the umbo (Figure 3d). Functionality is immediately verified using a Light Pen, which uses laser pulses to activate the Lens and provide a high-fidelity musical preview of the Earlens Light-Driven Hearing Aid for the patient.
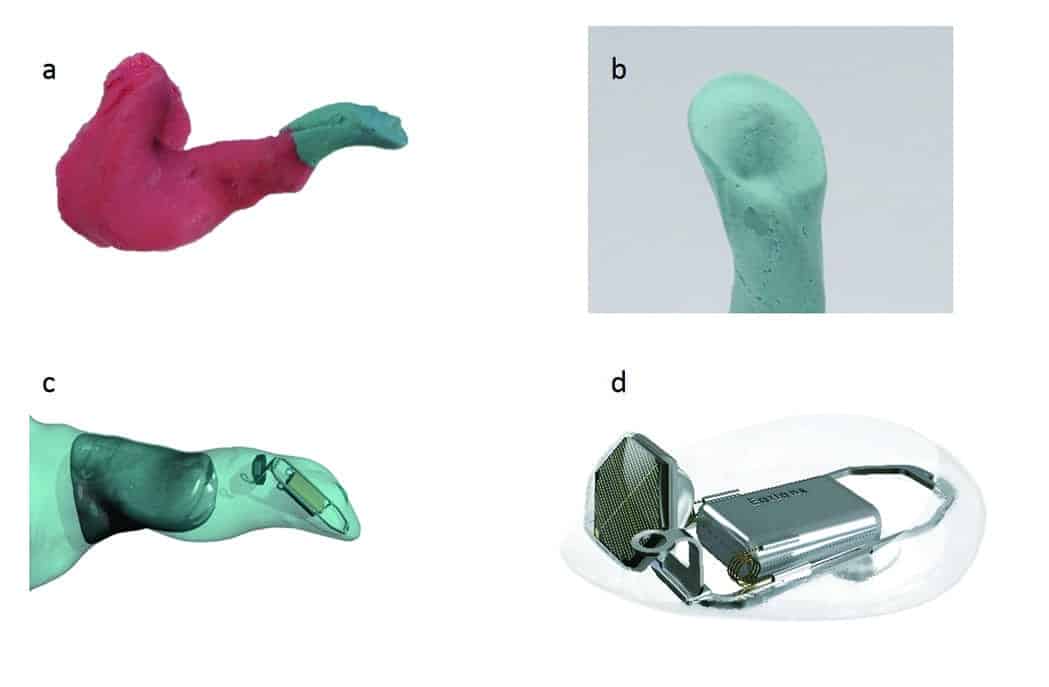
Figure 3. a) An example of a full impression taken by the ENT physician which includes the contours of the eardrum; b) A close-up example of an impression of the surface of the eardrum to which a Lens is customized in order to vibrate the umbo; c) Example of the digital modeling process which aligns the light emitted from the custom Light Tip with the photodetector on the Lens for each anatomy; d) Close-up of a custom Lens, depicting the photodetector, motor, and custom platforms which retain the proper position to drive the umbo.
The patient is then seen by the audiologist for calibration, fitting, and fine-tuning of the Processor and custom Light Tip. For the most part, the process is similar to the fitting and fine-tuning of an acoustic hearing aid. A key difference, however, is that the output calibration of the Earlens Hearing Aid is individualized for the patient via a process referred to as “light calibration,” as explained in greater detail below.
7) How are gain targets determined for the patient?
The Earlens fitting software uses the CAM2 prescriptive algorithm, an approach that is based on the concept of loudness normalization. This approach was developed at the University of Cambridge with the intention of restoring the overall loudness of sounds to the normal range while balancing the perceived loudness across frequencies. This approach is broadly applicable for speech, music, and other important sounds,10 and decreases the occurrence of harsh or tinny sound-quality complaints. When a broad bandwidth is achieved with CAM2, patients commonly report comfortable loudness and natural sound quality. As a result, in most cases, only minor fine-tuning of the high frequencies is required to arrive at acceptable patient settings.
8) How is the Earlens Hearing Aid calibrated to the patient’s ear?
Unlike acoustic hearing aids, the Earlens Light-Driven Hearing Aid is individualized to the user’s ear using an in situ calibration step in the fitting process called “light calibration.” Conducted by the audiologist in the first few minutes of the fitting appointment, this measurement establishes the baseline output calibration of the system on the individual ear, similar to the process of determining stimulation thresholds in cochlear implant systems. To the audiologist and patient, the process consists of audiometric threshold measurements where the Earlens Hearing Aid serves as the transducer.
Light calibration data is then used to align the output of the system with the acoustic reference point of the individual’s audiometric threshold at standard frequencies, ensuring that the data displayed on-screen in the fitting software is an accurate representation of the real-ear response for soft, average, and loud speech. The output curves displayed on the fitting screen are reflective of the actual output on the patient’s individual ear because the measurements incorporate the effects of the outer, middle, and inner ear, rather than relying on estimates of real-ear transfer functions.
9) Wait a minute… how do you know that the on-screen output is correct? And how do you verify the output without real-ear measures?
The required stimulation patterns necessary to generate perception of complex sounds at equivalent levels to acoustic stimulation were determined for the Earlens Hearing Aid based on experiments conducted on donated human temporal bones. With each light calibration measurement, the response threshold to light stimulation is matched to the audiometric acoustic threshold, scaling the output of the system accurately for the middle-ear energy transfer function of each patient’s unique ears.11
As further confirmation of the achieved output calibration, clinical verification measurements have been conducted in multiple clinical studies of the Earlens Hearing Aid.8-9 These measurements consisted of unaided and aided sound-field thresholds, which were used to calculate the functional gain. Functional gain is a close approximation to insertion gain at compression threshold, which allows comparison to the audiogram-based insertion gain targets for soft speech.12 The overall match to targets for higher level inputs can be confirmed electrically, as compressor function has been verified in temporal bone studies of the Earlens Hearing Aid.
Finally, a method of test box verification is under development that will allow the clinician to perform a “simulated real-ear measurement” and match to fitting targets in a hearing aid test box. This will approximate the widely accepted real-ear-to-coupler difference (RECD) fitting approach.13
10) What’s the three-sentence summary of this article and how do I learn more?
The Earlens Light-Driven Hearing Aid provides patients and clinicians with an amplification option that produces superior sound quality and extended bandwidth relative to traditional acoustic hearing aids. The system incorporates the unique characteristics of the outer, middle, and inner ear of each patient into the fitting process with a familiar look, feel, and process for the clinician. This technology is dispensed by an audiology and ENT physician team and represents a unique and significant step forward in the hearing device industry.
Readers can visit www.earlens.com for more information, instructions for use, and links to instructional videos.
Correspondence can be addressed to HR or Dr Dundas at: [email protected]
Original citation for this article: Dundas D, Carr Levy S. The Earlens Light-Driven Hearing Aid:
Top 10 questions and answers. Hearing Review. 2018;25(2):36-39.

References
-
Turner CW, Henry BA. Benefits of amplification for speech recognition in background noise. J Acoust Soc Am. 2002; 112(4):1675-1680.
-
Hornsby BWY, Ricketts TA. The effects of hearing loss on the contribution of high- and low-frequency speech information to speech understanding. J Acoust Soc Am. 2003; 113(3):1706-1717.
-
Carlile S, Schonstein D. Frequency bandwidth and multi-talker environments. Proceedings of the 120th Convention of the Audio Engineering Society. 2006; 118(1):353-363.
-
Plyler PN, Fleck EL. The effects of high-frequency amplification on the objective and subjective performance of hearing instrument users with varying degrees of high-frequency hearing loss. J Speech Lang Hear Res. 2006;49[June]:616-627.
-
Levy, SC, Freed DJ, Nilsson M, Moore BCJ, Puria S. Extended high-frequency bandwidth improves speech reception in the presence of spatially separated masking speech. Ear Hear. 2015;36(5)[Sept-Oct]:e214-e224.
-
FDA permits marketing of new laser-based hearing aid with potential for broad sound amplification[news release]. Silver Spring, MD: US Food & Drug Administration; September 29, 2015. https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm464839.htm
-
Struck CJ, Prusick L. Comparison of real-world bandwidth in hearing aids vs Earlens Light-driven Hearing Aid system. Hearing Review. 2017; 24(3):24-29. https://hearingreview.com/2017/03/comparison-real-world-bandwidth-hearing-aids-vs-earlens-light-driven-hearing-aid-system/
-
Gantz BJ, Perkins R, Murray M, Carr Levy S, Puria S. Light-driven contact hearing aid for broad-spectrum amplification: Safety and effectiveness pivotal study. Otol Neurotol. 2017; 38(3)[Mar]:352-359.
-
McElveen J, Gantz B, Perkins R, et al. Overcoming high-frequency limitations of air conduction hearing devices using a LIGHT-DRIVEN contact hearing aid. Poster presentation at: The Triological Society, 120th Annual Meeting at COSM, April 28, 2017; San Diego.
-
Moore BCJ, Glasberg BR, Stone MA. Development of a new method for deriving initial fittings for hearing aids with multichannel compression: CAMEQ-HF. Int J Audiol. 2010;49(3):216-227.
-
Puria S, Maria PLS, Perkins R. Temporal-bone measurements of the maximum equivalent pressure output and maximum stable gain of a light-driven hearing system that mechanically stimulates the umbo. Otol Neurotol. 2016;37(2)[Feb]:160-166.
-
Kuk F, Ludvigsen C. Reconsidering the concept of the aided threshold for nonlinear hearing aids. Trends Amplif. 2003;7(3):77-97.
-
Moodie KS, Seewald RC, Sinclair ST. Procedure for predicting real-ear hearing aid performance in young children. Am J Audiol. 1994;3[Mar]:23-31.




Years go by, and no answers! So typical – the attitude of the entire industry is just “shut up and give us your money!”
How much is it cost?
Nothing is mentioned about speech discrimination in severe sensory neural deafness with 100 decibel loss. Also is it suitable for perforated tympanum?
How will these work with mbl-phones ?
Presently using a plantonic device
Blu-toothed linked to my mbl-phone.