Practice Management | March 2018 Hearing Review
Practice strategies for the age of Medicare Advantage and DTC hearing aids.
The hearing healthcare landscape is changing, but there are several ways to not only survive but thrive in this new age including Medicare Advantage programs and constantly improving direct-to-consumer hearing devices. Part 1 looks at practical pathways for shifting to a fee-for-service (unbundled) business model.
At its core, the practice of audiology is a unique blend of the medical and retail. Because of state licensing requirements and academic training, audiologists, by definition, play a vital role in the diagnosis and treatment of ear disease and communication disorders. Research indicates, for example, that when the basic test battery is faithfully executed, audiologists are the appropriate entry point for patients with symptoms related to possible ear disease.1
Alternatively, there is a strong retail bend to the practice of audiology. This side of the profession centers on the sale of hearing aids, which are more apt to be perceived by the public as consumer electronic products than medical devices. Even though hearing aids have been regulated as medical devices by the US Food and Drug Administration (FDA) for more than 40 years, to the consumer—who is exposed to competitive advertising of these products and usually must pay a substantial portion of their retail cost out-of-pocket—hearing aids are often perceived as being more like laptop computers and headphones than artificial limbs or pacemakers. Audiologists, in turn, have adapted a bundled model and placed the hearing aid at the center of the bundle, and, for more than 40 years, charged a single fee for a comprehensive assortment of services that accompany the product.
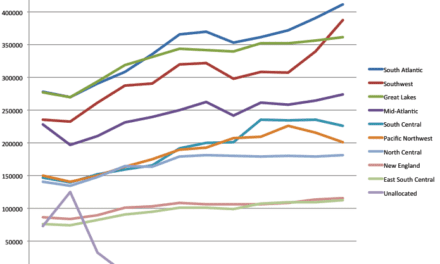
Historically, for a variety of familiar reasons, hearing aids have been purchased by around 25% of the potential market.2 Fortunately, given this poor market penetration and relatively low volume, it is the high margin of hearing aids that have kept many practices profitable over the past decades. This assertion is based on evidence, much of it anecdotal, suggesting that approximately 80% of the revenue generated in the typical audiology clinic comes from the sale of hearing aids, with the remaining 20% of revenue derived from diagnostic testing.3 Now, this successful business model—one based on the sale of a relative few number of units at a high margin—is at risk and looks likely to change.
There are two major forces driving this change: the rise of Medicare Advantage programs, and the increased availability of non-custom amplification devices sold directly to consumers. Medicare Advantage (also called Medicare Part C) plans are private insurance plans that serve as alternatives to the traditional government-funded Medicare program. Due to the aging baby-boomer population, Medicare Advantage programs now cover almost 20 million individuals, with a very high percentage of the people covered by this plan likely to have communicatively significant hearing loss.4 Because several private Medicare Advantage programs compete for the business of Americans aged 65 and older, a hearing aid benefit offered as part of any Medicare Advantage program is very attractive to members. Thus, there are now at least a half-dozen Medicare Advantage programs offering hearing aid benefits, often provided with a substantial reduction in margins for the practice.
Concurrently, hearing care professionals are witnessing a rise in the availability of high-quality personal sound amplification products (PSAPs) and other amplification devices sold directly to consumers. In the future, consumers are likely to have several self-fitting over-the-counter (OTC) hearing aids available at a range of prices. These direct-to-consumer (DTC) products are likely to alter (in some yet-to-be-determined way) the current hearing aid service delivery model.
Because of these forces, the 80-20 revenue blend of retail (hearing aids sales) and medical (diagnostic testing) services is likely to change over the next few years. Further, as all of healthcare becomes more consumer-driven—with a focus on lowering costs, increasing access, and improving outcomes—hearing care professionals must embrace a future that includes unbundling service fees from the sale of hearing aids. Even if your practice is profitable today using a bundled-fee structure, market forces soon may require a shift to an unbundled model to stay competitive. Here are four ways to get ahead of the curve.
1) Create a Culture Centered on the Use of Evidence-based Practices
The concept is simple: following evidence-based practice principles during the delivery of patient care adds a level of scientific rigor that cannot be duplicated by every licensed professional. But there is an inherent downside: it’s extremely difficult to get a team of providers working in the same clinic to agree on exactly which evidence-based practice principles will be used by the team. That’s where effective managers must fill the void by creating a culture where evidence-based practice is embraced and becomes part of routine care.
As more high-quality PSAPs and self-fitting hearing aids reach the market, audiologists must identify ways to differentiate the services they provide. After all, it is not a fantasy to think that some of the routine services that audiologists provide, like hearing testing and fine-tuning hearing aids, could be replaced by computer-based algorithms driven by machine learning and artificial intelligence placed in the hands of consumers. Simultaneously, a substantial number of patients who decide to go the do-it-yourself route will eventually need intervention from a hearing care professional. To continue to add value and avoid the commoditization of their professional services, audiologists should ensure that every test, procedure, and counseling session they conduct in the clinic contributes to an improved outcome for the patient and has a fairly priced fee connected to it .
Many audiologists have known the value of evidence-based practice for several years.5 Every professional organization has assembled a task force that has meticulously created clinical protocols based on a systematic review of research. For example, the American Academy of Audiology (AAA) created a clinical protocol for dispensing hearing aids in the adult population in 2006.6
It appears these evidence-based protocols are relatively easy to create, but are difficult to execute. One essential role of the clinical manager is to be familiar with these evidence-based protocols, clearly articulate their value in patient care, and obtain buy-in from staff members so the protocols become part of routine care. (To learn more about the role of managers in the execution of an evidence-based protocol see Nielson and Taylor, 2017.7)
A prime example of use of an evidence-based clinical protocol in an unbundled service model is the utilization of probe-microphone measures to evaluate the quality of a non-custom amplifier purchased off the Internet by a patient who is now in your practice. Let’s say a patient who self-fitted a PSAP seeks expertise from you. A probe-microphone analysis of the product in situ could be conducted, and the patient provided with an opinion about the quality of the fitting based on this measurement. Additional counseling time could be spent with the patient, addressing useful self-management techniques for better listening. For this 30-minute block of time you would charge a fee. But how much?
2) Calculate Your Clinical Rate Per Hour and Utilize a Superbill of Services
To know how much to charge for these type of services, the clinic must account for all expenses, including the salary of all providers directly involved in the care of patients. Once these expenses are calculated, the number is divided by the total number of patient contact hours, which is typically 6 to 7 hours per day for an entire calendar year, minus vacation, holiday, and sick time. Included in this calculation is a marginal profit of around 15% to 20%. This number is your clinical rate per hour. (To learn more about calculating a clinical rate per hour, see Coverstone8 and Quall9).
Once this per-hour clinical rate is calculated, it can be used to set prices for the delivery of all services. It can also be used to determine if third-party contracts will be profitable for your practice. Let’s use a round number of $100 per hour, which is much lower than the real-world rate you are likely to calculate. In this scenario, any 15-minute appointment, such as a hearing aid check, would be $25, and a 1-hour consultation would be $100. Finally, these rates would be applied to a superbill that lists all services provided by the practice.
Finally, this step culminates in the creation of a list of billable services with a corresponding CPT code (if applicable). Beyond fees and codes for typical items, such as audiological assessment procedures, hearing aid assessment and fitting procedures, and hearing aids (HCPCS Level II Codes), audiologists should consider adding additional services, such as counseling sessions broken into 15-minute time increments, some of which may require a patient to pay out-of-pocket. (For an example of an editable superbill, visit: https://www.audiology.org/sites/default/files/PracticeManagement/201105_AcademyEncounterForm.pdf)
3) Don’t Leave Money on the Table!
Moving toward an unbundled fee-for-service approach opens the door to collecting business from a wider range of patients in need of service, including those who purchased product elsewhere but need some level of professional assistance. However, the downside to an unbundled model is the potential loss of some of the large margins associated with the current bundled hearing aid-pricing structure. Therefore, practices moving toward a more unbundled model must ethically collect every dollar of revenue, either from third-party payers or out-of-pocket customers.
There are experts who can provide a clinic with the following information in granular detail about third-party contracts. Among the most frequent advice is to read the entire contractual agreement from the third-party payer and ensure that it includes a description of covered services and products and uses a current fee schedule with procedure codes for all services and products. One resource for learning more about billing and coding is Debra Abel’s new book, The Essential Guide to Coding in Audiology Coding, Billing, and Practice Management from Plural Publishing (2017).
Reimbursement from third-party payers doesn’t end with negotiating rates and managing the details of insurance contracts. Frontline service professionals are directly involved in the execution of third-party contracts, and in a fee-for-service model, precise execution of coding, billing, and credentialing will become even more important. For example, front office staff (eg, receptionist or patient care coordinator) must acquire insurance information before the patient’s appointment. Your clinic needs a clear process in place to ensure this is completed in a precise and timely manner.
Although a manager is likely to delegate these tasks, the following need to be taught to front office professionals:
- Obtain all current third-party payer information from each patient prior to their appointment with the audiologist;
- Verify coverage from the third-party payer prior to the patient’s appointment with the audiologist, and
- Clearly communicate to the patient in writing their out-of-pocket portion of the expense before any service or hearing aid purchase agreement is signed by the patient.
So far, the focus of this article has been on the jobs of managers, working behind the scenes, ensuring the business runs smoothly, and optimizing cash flow through proper pricing, billing, and collection. Now, let’s turn our attention to the work of the clinician—the highly trained expert who blends art and science to treat hearing loss. None of the items mentioned previously are useful unless the clinician can deliver a service valued by consumers.
4) Right Service, Right Time, Right Personnel: Unbundling Begins with Triaging Routine from the Complex
A shortcoming of the existing bundled audiology business model is that, for the consumer, it appears everyone is receiving the same type of service—regardless of actual need. As we move into the future, a bundled business model is problematic because some patients will require diverse types of professional services than what is currently provided in a clinic that bundles services with the delivery of hearing aids.
With respect to professional services, often the only variable in a bundled audiology business model is the amount of time spent with each patient. Often, this is an unpredictable variable. When professional services are bundled with the sale of a product, it leads to a highly inefficient situation in which the complex patient, who takes more time to help, is subsidized by the routine patient, who requires very little clinical time to have their needs met. To further aggravate the situation, both types of patients in the current bundled business model usually pay the same retail price.
For an unbundled service model to be profitable, hearing care professionals should find ways to deliver the right type of service (counseling) for the right amount of time, using personnel with the right level of training for the job at hand. Fortunately, we have some examples to help guide the way to a more efficient service delivery model with unbundled prices. About 10 years ago, two European research audiologists, Dafydd Stephens and Sophia Kramer10 created a patient classification system focused on the emotions, attitudes, and maladaptive behaviors of the patients with hearing loss. It is a system based on categorizing adult patients as one of four types, with 80% to 90% of patients fitting into either the Type 1 or Type 2 categories shown in Table 1.
To properly categorize patients into one of the four types requires hearing care professionals to employ more novel approaches to stratifying communication disorders into routine and complex cases, with those deemed complex requiring more time and expertise to remediate. Toward that end, what follows is a new and yet-to-be-proven approach that warrants consideration.
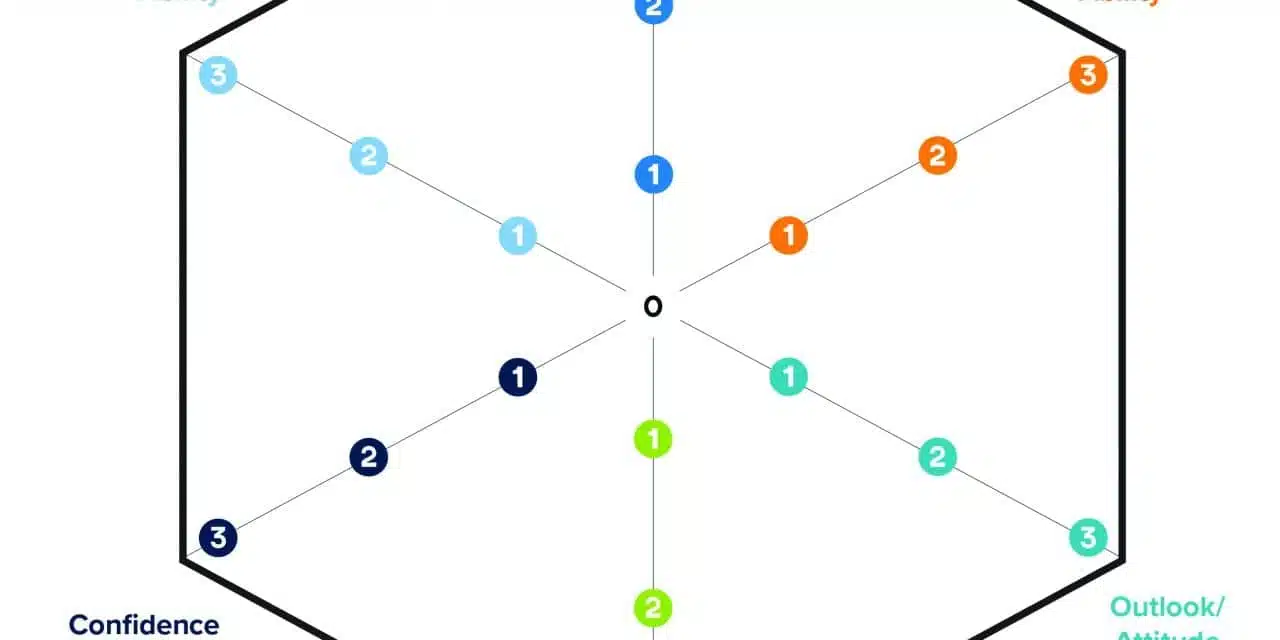
The six dimensions of adult patient hearing care shown in Figure 1 have a direct impact on the outcome of care. All six of these dimensions cannot be assessed with traditional audiological assessment tools (eg, pure-tone air and bone-conduction audiometry or speech testing). For purposes of discussion, these six dimensions are referred to as “non-audiological components of care,” and, as any practicing clinician knows, each dimension influences the outcome and the amount of clinical time required for successful aural rehabilitation. In addition, the rating of each of these six dimensions determines the type/amount of necessary service provision.

Figure 1. The Communication Hexagram is a tool providers and patients can use to rate six important dimensions affecting service provision options and treatment outcomes.
- Cognition: The executive intellectual function (memory, language comprehension, etc) of the individual.
- Physical ability: The dexterity of the individual, particularly fine-motor and haptic (sense of touch) ability.
- Attitude and motivation: The general outlook of the individual toward life, but this also includes outlook toward completing new tasks or changing/modifying behaviors needed to be a successful communicator. When judged on a continuum, the individual could be stubborn to compliant or extremely optimistic to extremely pessimistic.
- Family Support: Consistent contact with either a family member or close friend (communication partner). On the opposite side of the family support continuum, would be social isolation.
- Self-confidence: Trust in one’s abilities and judgements in completing a task or modifying a behavior per the recommendation of a professional. Self-confidence can influence a patient’s ability to succeed in learning all the new tasks associated with a recommended treatment.
- Self-perception of hearing loss: An individual’s own judgement or awareness of their ability to hear and its associated handicapping condition. Oftentimes, a clinician can assess self-perception of hearing loss by asking a scaling question (“On a scale of 1 to 10, with a 10 being perfect hearing, how would you rate your overall ability to hear?”).
The professional’s ability to assess each of these non-audiological components of care—either formally, with a validated self-report, or through informal observation—is an opportunity to get the patient and their communication partner involved in the appointment process. During the assessment process (assuming there are not any medically complicating factors), the audiologist would lead a discussion about each of the six dimensions. If there is a discrepancy between the patient and the audiologist of more than 1 point, or if the audiologist gives a rating of 0 or 1 for any of the six dimensions, that dimension would be considered a complicating factor (ie, a Type 2, 3, or 4 condition). This evaluation process occurs before treatment (eg, hearing aid use) begins; therefore, pathways to a successful outcome can be communicated to the patient and communication partner.
Table 1 summarizes the likely next steps of this assessment process. Notice that the Type 1 condition’s result is the same type of care continuum that occurs today: the patient is fitted with hearing aids and returns for a series of rather quick routine, follow-up appointments. Type 2 patients are also likely hearing aid users; however, complicating factors necessitate additional appointments (or longer appointment times) to address these complications. For example, if the patient is judged to have poor self-confidence that is precluding his ability to be a successful hearing aid user, additional appointment time is spent, with the audiologist focusing on tactics to support the patient. Patients are charged accordingly for the clinical time and know in advance this will be a focus of their appointment(s).
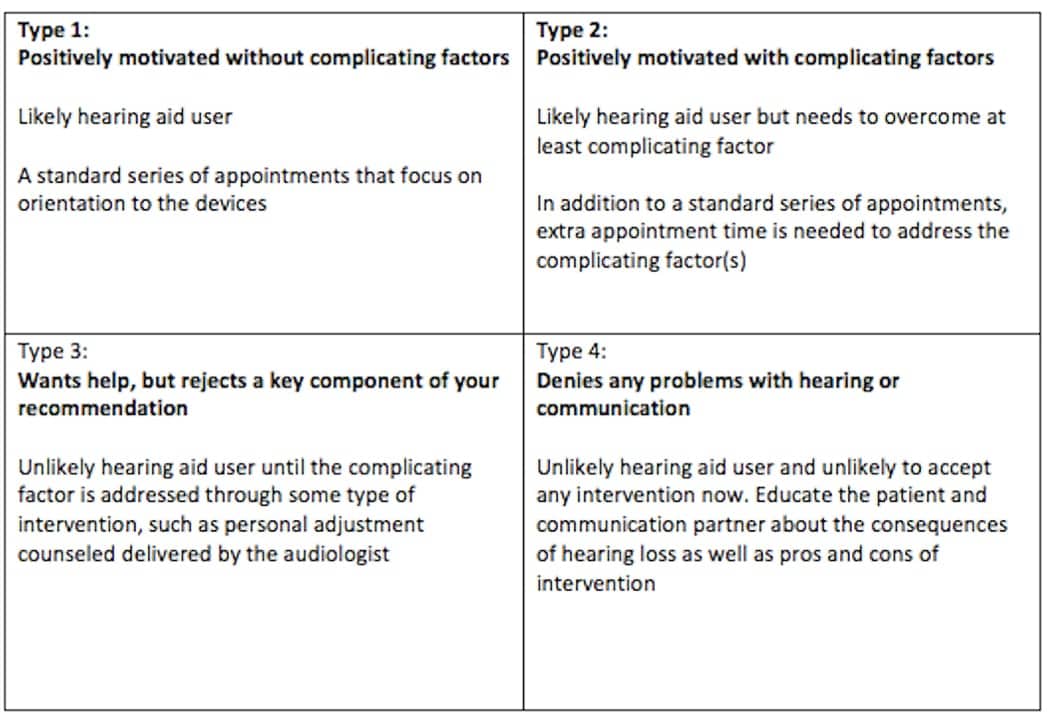
Table 1. A summary of likely next-step options for each of the four condition types outlined by Stephens and Kramer.10
Type 3 and Type 4 conditions warrant special consideration because it is likely both types of patients will not be immediate hearing aid users. However, because clinical time can be spent addressing why a patient might be rejecting a treatment recommendation, they could be provided with a service, such as personal adjustment or self-management counseling. An accompanying fee would be charged, too. Moreover, Type 3 and Type 4 patients who have been identified as needing help could possible benefit from a trial with a non-custom amplification device or additional personal adjustment counseling—both provided by the audiologist for a fee.
Conclusion
The main objective of “Ahead of the Curve #1” is to provide a logical pathway for shifting to a fee-for-service business model. Innovative approaches to patient care are required for audiologists to stay competitive as their practice landscape quickly changes. The market need for hearing care offices to provide exceptional value (and a competitive advantage) is directly tied to the execution of proven evidence-based practice protocols. Audiologists who are poised to adapt to new business and clinical practice models will differentiate their practices based on service and be successful over the long haul.
Audiology will continue to involve some combination of medical and retail work. Market forces, however, are likely to determine how each of these components are packaged and sold to consumers in the future. Ahead of the Curve #2 will focus on self-management skills in older adults and the opportunity this assessment method holds for those hearing care professionals willing to provide more counseling services that are unbundled from the sale of hearing aids and other amplification products.
Correspondence can be addressed to HR or Dr Taylor at: [email protected]
References
-
Zapala, DA, Stamper GC, Shelfer JS, et al. Safety of audiology direct access for Medicare patients complaining of impaired hearing. J Am Acad Audiol. 2010;21(6)[Jun]:365-379.
-
Staab, W. Hearing aid market penetration. December 9, 2014. Available at: http://hearinghealthmatters.org/waynesworld/2014/hearing-aid-market-penetration/
-
Strom KE. HR 2013 hearing aid dispenser survey: Dispensing in the age of internet and big-box retailers. Hearing Review. 2014;21(4):22-28.
-
Nolden T. Medicare Part C–Medicare Advantage. August 2, 2017. Available at: https://medicare.com/medicare-advantage/medicare-part-c
-
Kochkin S, Beck DL, Christensen LA, et al. MarkeTrak VIII: The impact of the hearing healthcare professional on hearing aid user success. Hearing Review. 2010;17(4):12-34.
-
Valente M. Guideline for audiologic management of the adult patient. October 30, 2006. Available at: https://www.audiologyonline.com/articles/article_detail.asp?article_id=1716
-
Nielson D, Taylor B. The need to succeed: How to navigate the transition from clinician to director. Audiology Practices. 2017;9(4):20-25.
-
Coverstone JA. 20Q: Fee-for-service in an audiology practice. March 5, 2012. Available at: https://www.audiologyonline.com/articles/20q-fee-for-service-in-776
-
Quall D. How low can you go? Practical considerations when offering a low-priced hearing aid [webinar]. March 23, 2016. Available at: https://hearingreview.com/2016/03/webinar-low-can-go-practical-considerations-offering-low-priced-hearing-aid
-
Stephens D, Kramer SE. Living with Hearing Difficulties: The Process of Enablement. Wiley-Blackwell: West Sussex, UK; 2010.
Citation for this article: Taylor B. Getting ahead of the curve, part 1: Four cornerstones of a fee-for-service clinic. Hearing Review. 2018;25(3):16-20.