
Research | April 2019 Hearing Review
Individual perspectives on how UHL affects their daily lives, attitudes, and relationships
There is a need to improve awareness and to better understand the impact and struggles of people who have unilateral hearing loss (UHL), the professionals who treat them, and those who work, live, and socialize with them. With better awareness comes better understanding, so health professionals can refer them rather than dismiss them. Moreover, better understanding can fuel motivation and allow the person with UHL to be more proactive about managing the condition while reducing anxiety.
Unilateral hearing loss (UHL) has been defined as a 3FA pure-tone average (PTA) above 20 dB HL or thresholds above 25 dB HL at two or more frequency above 2 kHz in the affected ear.1 UHL in adults has an estimated prevalence of 7.2% of the overall population, with only 2% of people with UHL using a hearing aid or device.2
Some of the effects of UHL have been established in the literature, including difficulties to understand speech in background noise and reduced spatial awareness.3,4 In our research, we wanted to explore individual perspectives of the impact of UHL on people’s daily lives and the difficulties encountered, to provide a better understanding of the unmet needs of this population.
Methods
A 6-person research team at the National Acoustic Laboratories (NAL) explored this area using two qualitative approaches:
1) Semi-structured interviews were conducted in person or via phone/Skype with 14 adults who had unilateral hearing loss. They were either invited to participate from a volunteer research database or responded to a flyer invitation to participate. All interview participants provided written or verbal consent prior to taking part.
2) An open-ended survey consisting of questions that complemented those asked in the interviews was designed to capture responses from a wider audience. An invitation to complete the survey was posted on public forums specific to UHL, such as the Action on Hearing Loss forum and relevant Reddit threads.
The interview and survey questions were grouped into six main categories:
- Participant’s background information;
- Awareness and the causes of UHL;
- The impact of UHL;
- Treatment decision-making (in this case, treatment refers to the use of a hearing device of any type);
- The implications of treatment or no treatment, and
- Suggestions and needs.
Information from interviews and surveys were combined and main themes identified, which are discussed below.
Results
Demographics. A total of 14 adults with UHL participated in interviews, and 80 adults (34 females, 46 males) responded to the survey, including 17 from the Australian Hearing database, 51 from reddit, and 12 from the Action on Hearing Loss forum. Participant ages ranged from 18-71 (mean: 34.9). Among these participants, 53% were located in the United States/Canada, 31% were from Australia, and the other 16% were from other countries (eg, Netherlands, Vietnam, and India).
The causes for the UHL were diverse including meningitis, head trauma/accident, absence of auditory nerve, tumor, otosclerosis, microtia/atresia, Ménière’s disease, virus, mumps, noise exposure, and measles. Among these participants, 44% reported currently using a hearing device, and 32% reported that hearing loss was identified since birth.
Trends, Themes, and Stories
Congenital vs acquired UHL. Responses from the interviews and surveys presented a clear difference between the experiences of those with congenital and acquired UHL. Those born with UHL were more likely to have developed excellent coping mechanisms (ie, placement, lip reading, etc), and perceived less impact on their quality of life. These congenital UHL respondents were also more likely to find the devices to be an annoyance or hindrance, and many who were prescribed devices chose to discontinue their use, often deciding that they were coping fine without them. For example, one congenital UHL participant said, “Nothing is particularly frustrating. Having been unable to hear in one ear all of my life, I just deal with it.”
In contrast, those with an acquired UHL reported that it had a greater impact on their quality of life. They commonly described experiencing panic at the onset of hearing loss, and because of this they were quick to seek treatment. They also had to deal with grief, having lost the functional benefits of binaural hearing and potentially losing elements of their former lifestyle. Most respondents struggled with adjusting to the change and with accepting the consequences of their condition.
Acquired UHL participants commonly reported having tried contralateral routing of signals (CROS) hearing aids, and less commonly implanted devices such as a bone-anchored hearing aid and cochlear implants (CIs). While some participants gained benefit from CROS in some scenarios, these devices tended not to provide much benefit with speech understanding in high noise situations or with localization—the two primary hearing related issues for this population.
Tinnitus and UHL.There were a number of participants who reported having tinnitus, and usually this was a major problem for them. For example, one participant stated,“The tinnitus is worse than the hearing loss and has affected me more negatively than the hearing loss itself.”
A total of 29 themes/situations were identified in which participants experienced difficulty because of their hearing loss. The themes are further divided into three categories: 1) Functional impacts, 2) Psychological impacts, and 3) Social/behavioral impacts.
1) Functional Impacts
Listening in noise and localizaton. The two most commonly reported functional impacts were difficulty listening in noise and poor localization. Participants reported having the most difficulty in loud environments and when there were lots of sound sources. One respondent stated, “Conversations can be unbearable, especially in loud places,” and another added, “I find it hard to listen when large groups of people are together and talking over each other.”
Many participants reported difficulty recognizing the direction from which sounds came from, often perceiving that all sound sources originated at their good ear. For example, one participant said, “I have a hard time telling what direction sound comes from if I can’t see the source of the noise.”
Respondents noted they had difficulty hearing sounds on their poor side, such as one who said, “Scenarios where I need to hear someone on my deaf side are extremely frustrating and sometimes totally impossible.” Some respondents also mentioned having auditory blind spots, including a subject who said, “I feel almost like I’m blind on the left because I have no sense of someone being there and certainly can’t hear them.”
There were also a wide range of scenarios in which people reported functional difficulties, including listening while in a car, enjoying music, and playing sports and video games. One positive theme was that participants reported better sleep, as there was less background noise with their good ear pressed against the pillow. However, this was also seen in a more negative light with respect to difficulty being woken up from sleep, which may be important in an emergency.
Fatigue. Participants also reported experiencing fatigue from the increased cognitive load required during activities such as conversation in loud noise. One participant said, “By the end of the meal, my brain is usually exhausted from trying to hear everyone.”
2) Psychological Impacts
Fear/anxiety. Most interviewees and survey respondents indicated that their mental health was impacted by their hearing loss. People expressed emotions such as fear in various ways. One example of this was the perception that the person’s safety, or the safety of those around them, might be at risk due to their hearing impairment. One respondent stated,“I’m concerned about being in a situation where someone I love is in danger and my directional hearing affects it.” Participants were also afraid of losing hearing in their good ear and the potential further consequences of such a loss. Others feared familiar or social abandonment due to the perception that their UHL made them a burden or annoyance to those around them. One participant voicing this fear said, “I fear my good ear getting bad and all my friends and family slowly dropping me out of their lives.” Those with an acquired hearing loss also expressed panic, especially if the loss was sudden.
Participants also expressed feelings of anxiety, often over how others might judge or perceive them. One subject said, “I wish I could feel less anxious about being judged for misunderstanding or not hearing people,” while another expressed “anxiety over thinking that others think I’m ignoring them.”Another participant expressed general anxiety relating to their hearing loss: “I think it has created a lot more anxiety in me overall my whole life [sic]. I think the anxiety comes from lack of ability to place sound, so I’m not as comfortable as other people are in noisy situations.”
Self-esteem and difficulty in social situations. Some participants expressed having a poor perception of themselves, in which they felt like they were a burden to those around them, or felt anxious and self-conscious about their difficulties communicating. One participant described it as follows: “I can’t understand when they say things to me until I ask them to speak clearly and at me. It hurts me to think that they think negatively of me because of it.”
It was clear that hearing loss weighed heavily on them, resulting in feelings of depression and feelings of disconnection with the world around them. Participants reported feeling isolated from others and actively isolating themselves by avoiding social situations. The difficulties encountered in daily communication reduced the attractiveness of social gatherings. For example, one stated, “I think the social isolation is the worst. I very rarely socialize in noisy environments as it’s just too stressful and difficult.” Some people noticed that their hearing loss had changed their behavior:“I became an introvert, and don’t go out much.”
Participants commonly encountered frustration throughout their daily life, particularly in social situations. One participant reported frustration at having “to ask people to repeat themselves more often than most people,” while another at having “to constantly tell people who try to talk into my deaf ear that I can’t hear out of it and then explaining why.” Yet another respondent simply stated, “I have been frustrated with my disability all my life.” In some cases, the frustration described by participants included strong elements of distress, such as one person who said, “It makes me feel broken, like I can’t get simple instructions at work.”
3) Social/Behavioral Impacts
Reduced social engagement.Most participants mentioned having problems with communication in social situations, resulting in feelings of disconnection from the world around them. In some cases, these problems caused the individual to isolate themselves by avoiding social situations. Furthermore, participants reported engaging less in communication with their close family and friends due their difficulties. Participants’ hearing loss also affected their relationships with family in other ways; one participant described arguments that occur with his wife relating to his hearing loss: “I’ve been married for over 15 years, and I still get into arguments with my spouse because I missed something she said. I have an expectation that she would understand by now; she has an expectation that I can hear.”
Missing out on important information. Participants reported missing important information while in communication but also more trivial information such as jokes, which left them feeling as though they were missing out. As a result, participants often had to ask people to repeat themselves; this was a source of frustration for the participant and they also perceived it as being frustrating for those around them.
This perception of frustration meant that participants were discouraged from communicating their needs to others. One participant stated, “People think I’m ignoring them when really I can’t hear. People forget that I’m hard of hearing. People get easily frustrated that I can’t hear them.”
Participants suggested that societal awareness of UHL was generally poor, and perhaps those around them tended to become frustrated due to a lack of understanding and empathy. They felt that the “invisibility” of hearing impairment was a significant contributor to this, preventing those around them from relating to the difficulties they encounter during daily life.
Stigma in the workplace. One of the more commonly reported themes in this study was stigma. Participants reported having a strong perception of stigma, particularly in the workplace, where they did not want others to know and judge them for their hearing loss. This often affected participants’ behavior, such as wearing devices. For example, one participant said, “I only wear it on weekends. I don’t want my work to know about my disability.”Another participant noted, “I fear that if I have a hearing aid, people will automatically assume that I am fully deaf or incompetent to perform my job.”
A more general comment from one of the interviewees was, “I try not to mention it to people unless it’s really obvious.”
Coping mechanisms.Participants developed various coping mechanisms in response to the difficulties encountered because of their hearing loss. Participants recognized that, in some cases, coping mechanisms were applied through conscious effort, while in other cases they had adapted without conscious thought. Those with congenital UHL tended to develop coping mechanisms more easily and naturally than those with acquired UHL. There were a variety of coping mechanisms identified, including strategies to improve communication in noisy environments, such as lip reading, sign language, and favoring their good ear.
Other coping mechanisms required proactive action, such as positioning themselves in a corner of a room, or positioning themselves to have important sound sources on the side of their good ear while walking or at a table. More proactive coping mechanisms included communicating their needs with those around them, and moving to a quieter location before engaging in conversation.
The perception of stigma was a barrier to some coping mechanisms, as participants preferred not to disclose their hearing loss to others. As a consequence, another coping mechanism exhibited by participants was pretending to understand to avoid the awkwardness of repeatedly asking someone to repeat themselves.
Personality appeared to have an effect on the use of coping mechanisms and participant outcomes, with extroverted individuals being more likely to disclose their hearing loss to others and generally more comfortable being proactive about their hearing loss. Thus, extroverts had more positive outcomes than introverts.
Participants also mentioned using closed captions while watching television and using assistive smartphone applications/settings. Finally, some participants visually identified their deaf ear by wearing an earbud or having a tattoo, to encourage those around them to position themselves beside their good ear before engaging in conversation.
Technology/Devices
Untreated group comments. Figure 1 shows the main reasons for participants in the untreated group not choosing devices. Most participants (28%) reported that they did not use a hearing device because they thought that it was not useful or because they were told that it was not helpful. About 21% of the respondents reported they were coping well enough that they had no need to use a hearing device.
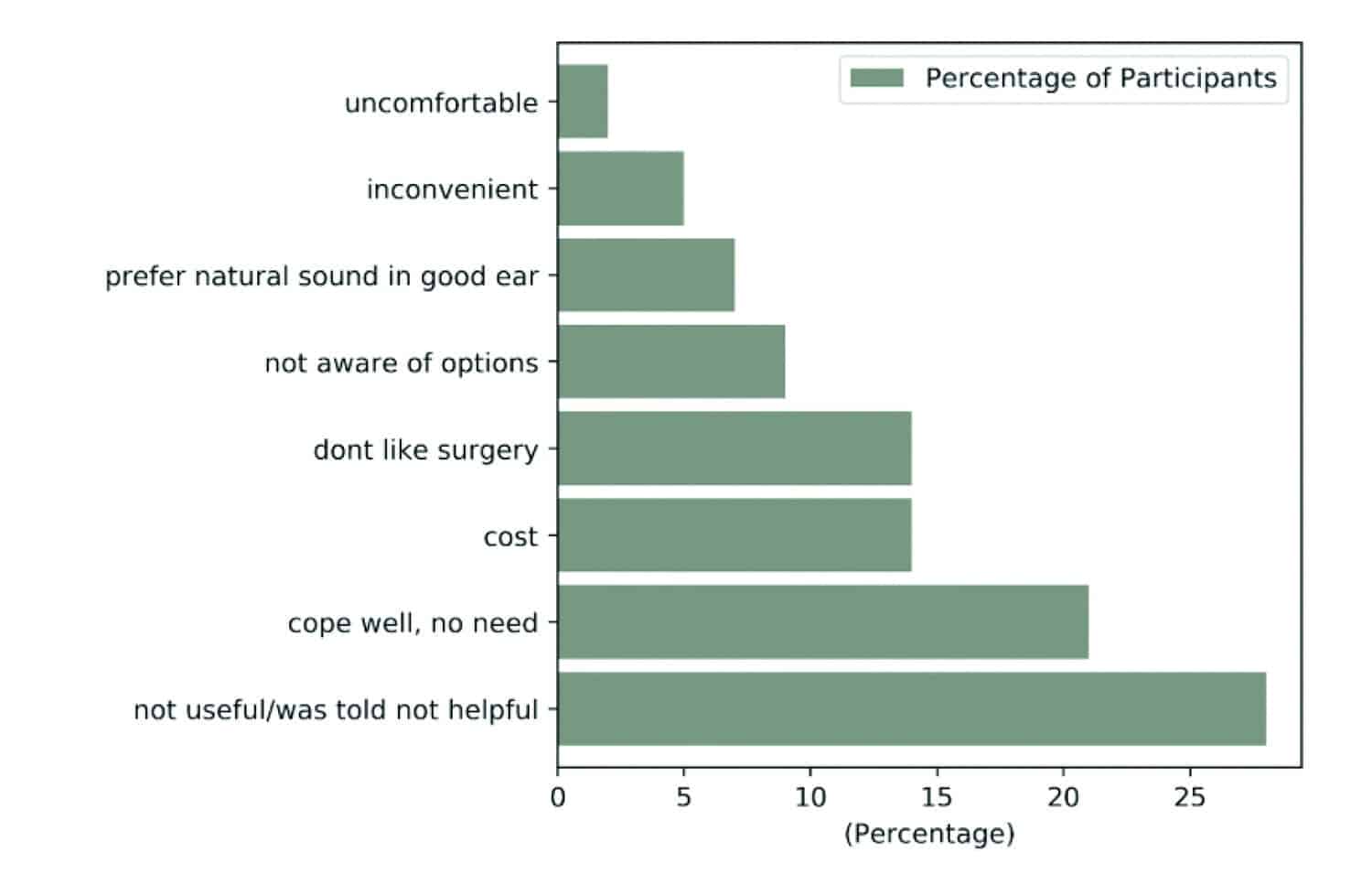
Figure 1. Main reasons for participants in untreted group not choosing devuces (n=50).
The cost linked to the hearing rehabilitation and the invasiveness of the treatment were another two main reasons (14% each) for not using a hearing device. This is especially true for people who don’t have any reimbursement available. Participants reported, “I do not like the idea of a surgical solution that leaves a lasting cosmetic impact. Waiting for technology to get smaller/better,”or said that it “seems intrusive for someone with a working ear.” Some participants were just not aware that rehabilitation options existed (9%).
A social stigma or negative perception about their hearing loss from others was also a common reason for not getting/wearing a device. A respondent told us, “I had anxiety in young age, victim of bullying and harsh comments. I gave up on wearing them due to these things.”
Treated group comments. Considering the treated group, adults with UHL reported variable degrees of benefit with hearing devices (Table 1). In general, half of the participants fitted with a bone-anchored device or CROS system reported being relatively satisfied with their hearing aids. However, while some enjoy using them—“great, made a big difference from the first aid fitted. I would wear 12 hrs a day and only take it out at night.”—others report dissatisfaction with currently available technology.
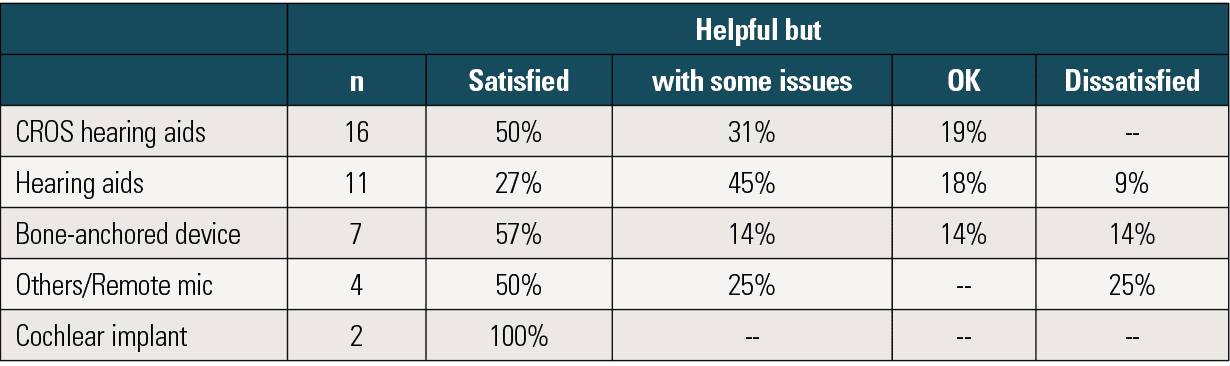
Table 1. Satisfaction with the different devices used by adults in the treated group.
A reported issue with the CROS system is its poor performance in noisy environments—“at parties or loud spaces it doesn’t offer much benefit”—and that it does not help localize sounds. Another complaint from the user was the negative effect of noise routed from the bad ear to the good ear, which affects the overall sound quality for the listener. Some of the comments from the CROS users included, “I use it whenever I am outside the house and most of the time provides significant help,” “It is definitely better than nothing,” “Useful in one-on-one or more intimate settings,”and “useful in relatively quiet situations.”
The bone-anchored hearing aid users’ satisfaction ranged from “very satisfied,” because it decreased listening effort, to “dissatisfied.” Positive comments from these users included “…being able to converse with people in public more easily,” “I got my energy back and I am able to to be more active. I can also now hear lyrics to songs,” “It helped my tinnitus,” and “It helps a lot with sound location, anytime I am in public, and I find it incredibly useful.”
Some of the comments from the hearing aid users included “It’s amazing and worth it. It just takes time,”“I use whenever I am out of the house, especially for loud and crowded places; it’s incredibly helpful in normal situations,” and “It makes hearing easier and conversations much easier to pick out of background noise. A standard hearing aid helps considerably. Outside of the house I use it ~80% of the time.”
There were only two CI users in the treated group. One of them had a trial with a hearing aid, a CROS, and a bone-anchored device, and they took the decision of cochlear implantation due to the lack of benefit using these devices. Although both of these participants were very satisfied with the CI option, more evidence of the outcome is needed.
Some comments from people using Bluetooth features were, “The Bluetooth features are incredible,” and “It uses a lot of the battery.”
People’s Wishes
As part of our exploration, we put forward two questions to tap into people’s wishes for the future:
1) What would you like to see or be using in the next 5-10 years to help your hearing?
2) If you could change/improve one thing that is related to your hearing loss, what would it be?
New technology, such as real-time audio captioning using Internet of things’ (IoT) devices were mentioned multiple times. People also mentioned “dreams of bionic implants to restore near perfect hearing,”and “hair cell generation.”
Related to the themes and trends we have discussed previously, the call for better awareness was made multiple times: “If I could change/improve one thing that relates to MY hearing loss, I would say better public understanding,” “I would like more recognition in society that single-sided deafness can be hard to deal with. I’ve never really had anyone understand how it’s a challenge in my life,” or simply the wish for “Compassion and empathy from other people.”
One respondent who struggled with anxiety around their hearing loss also expressed, “I wish I could feel less anxious about being judged for misunderstanding or not hearing people.”
Conclusion
It is important to understand the demographic limitations of the current study in terms of participant recruitment from an internal database for interviews and from online forums for surveys. Nevertheless, the relatively large age spread across participants and the wide variety of etiologies provides a good overview of the issues faced by adults who have a UHL.
Importantly, our analysis showed that the impact of UHL varies among individuals. While one-fifth of the people who took part in the study reported that they were coping well in general, the majority of participants reported a significant impact of UHL on their social life and on their well-being.
Another trend identified was the different perceptions regarding the burden of impact between people who suddenly acquired UHL—who reported stress, anxiety, and difficulties—and people born with UHL, who are better adapted and reported a larger variety of coping techniques.
The most common treatment reported for UHL was a CROS hearing aid. Some UHL patients used bone-anchored hearing devices and reported good benefits. Overall, however, our exploration found that these two devices do not seem to address localization or speech-in-noise understanding adequately. The inconvenience of the hearing devices (including the cosmetic features of the device) and the invasiveness of some of the treatment options are barriers to use or continued use, and may outweigh the perceived benefits.
Another emerging treatment option is a CI. However, there is limited evidence and information on the outcomes of this treatment for UHL—or the current evidence has not permeated through to general knowledge as yet. As for other treatment options, the invasiveness and the cost of getting a CI is a clear barrier that many people cannot overcome to consider this as a viable treatment option for them.
Lastly, we found that the psychological impacts of UHL are significant and varied, becoming the main focus within our exploration of this population’s experiences. Most importantly, there is a need to improve awareness and to better understand the impact and struggles of people who have unilateral hearing loss, the audiologists who treat them, and those who work, live, and socialize with them.
About the Authors: James Galloway, MDesSc (Audio & Acoustics), is a Research Engineer, Vicky Zhang, PhD, is a Research Pediatric Audiologist; Vivienne Marnane is a Research Speech Pathologist; Sanna Hou, MClinAud, is a Research Pediatric Audiologist; Greg Stewart is a Technical Support Officer, and Fabrice Bardy, PhD, is a Research Scientist at the National Acoustic Laboratories (NAL) in Sydney, Australia.
Citation for this article: Galloway J, Zhang V, Marnane V, Hou S, Stewart G, Bardy F. The impact of unilateral hearing loss on adult life. Hearing Review. 2019;26(4)[Apr]:10-14.
Correspondence can be addressed to Dr Bardy at: [email protected]
References
-
Centers for Disease Control and Prevention (CDC), Early Hearing Detection and Intervention Program and Marion Downs Hearing Center. Workshop Proceedings. Paper presented at: National Workshop on Mild and Unilateral Hearing Loss.Beaver Run Resort; July 26-27, 2005; Breckenridge, CO. https://www.cdc.gov/ncbddd/hearingloss/documents/unilateral/Mild_Uni_2005%20Workshop_Proceedings.pdf
-
Golub JS, Lin FR, Lustig LR, Lalwani AK. Prevalence of adult unilateral hearing loss and hearing aid use in the United States. The Laryngoscope.2018;128(7):1681-1686.
-
Firszt J, Reeder R, Holden L. Unilateral hearing loss: Understanding speech recognition and localization variability-implications for cochlear implant candidacy. Ear Hear.2017;38(2):159-173.
-
Lucas L, Katiri R, Kitterick PT. The psychological and social consequences of single-sided deafness in adulthood. Int J Audiol.2018;57(1):21-30.



It is good to know that I am not overreacting to impact of loss of my right ear. My solution is to see people 1:1 in quiet places. It was due to medical negligence. It has cost me my job ( I was a lecturer) as hearing aids are unsightly and I will not have them. No CROS: two sided solution for one sided problem.CI very visible and requires shaving of head. The only solution is to learn to live in isolation. See my parents and siblings at different times, friends drift away if you ignore their calls for long enough. Husband will not be far behind as I refuse to go to noisy places with him and I refuse to take medication to deal with social anxiety. The loss was not my fault and I am not polluting my body with drugs.. I had an amazing 54 years as a social creature and now want only my own company as I push for medical retirement from lecturing .
I’m sorry to hear these sentiments and your withdrawal from society. Everyone has, and is entitled to, their own opinions and can live the way they wish. However, I assure you that hearing aids (or even a cochlear implant) are MUCH less obvious than an apparently smart and engaging person like yourself who can no longer communicate well and interact with others. There is a hearing solution for almost ANY hearing problem. However, I understand that it’s the psychological barriers to hearing loss that are hardest to overcome. I hope you’ll come to find an amplification option that helps you re-engage with the world and your loved ones. My opinion is we’re social animals and we need personal contact for grounding, growth, support, and for a healthy and happier life. Good luck.
CIs are not very visible, especially for women. Many people hardly notice my husband’s anymore. Seems like everyone is walking around with some sort of Bluetooth device hanging on their ear! I’m sad to think of you or anyone giving up so many important relationships and experiences when there is technology that can help. My husband has had 1 CI for almost 20 years…I can’t imagine our lives without it. Go to a CI audiologist and learn about your options.
I was born with no hearing in my left ear and about a 25% loss in my right ear. When I was about 30 I got a hearing aid, which was quite helpful, but did nothing for the one-sided deafness. Recently I was fitted with a CROS aid it is very helpful, but not perfect, especially in social situations.
A few years ago I met a woman who, like me, was deaf in one ear. On meeting her I noticed that she had a wad of white cotton in one ear, which was very noticeable. She told me later that the cotton was not for medical reasons but to alert people that she did wouldn’t hear anyone speaking to her on that side. I thought that was very clever of her, and it was quite effective. So I want to pass along this tip to others with one-sided deafness. It worked for me, until I got a CROS aid.
My husband-69yo- just lost hearing in the left ear from an injury then virus.
Cotton ball in affected ear is a great idea.
Has been devastating for him. This paper is very helpful!
Thank you
Joyce
Thank you for the wonderful article! I am 27 years old and have been completely deaf in my left ear as long as I can remember. Because of that I have adapted well and coping mechanisms are as second nature to me as walking.
I am very extroverted and have always had a supportive group of friend and supportive family. That has made it so much easier over the years. They always save me a spot on the left side of the table, and when I switch sides with them while walking they don’t even mention it because they know why I’m doing it. I’ve never been directly embarrassed by my ear, but when I was a child I was embarrassed that I had to go to speech therapy classes even though no other kids gave me a hard time about it. I am very open with people about my unilateral deafness because I’ve found that it makes my mannerisms less awkward. People I don’t know well think it is awkward at first when I switch sides or turn myself to hear, but when I explain why I’m rearranging myself it suddenly is a lot less awkward and they usually think little of it.
Being unilaterally deaf certainly has its challenges though! I have a great deal of anxiety when talking on the phone. Talking on the phone makes me completely unaware of my surroundings. It also makes loud places far less enjoyable. When I’d go bar hopping in college with friends I wasn’t able to enjoy myself in the crowded bars, but was able to cope with it easily in the smaller bars without a lot of noise. It also is a huge inconvenience when I get an ear infection in my good ear. When my good ear has an infection it’s a huge deal and sometimes people don’t understand that. It’s impacted my learning and dating life as well. My friends have always been supportive, but sometimes it can make me seem awkward on first dates. Especially if those dates are at a restaurant or crowded place. They also have to understand that I don’t enjoy face-timing or phone calls because of my deaf ear. Once they get used to me it isn’t awkward anymore. It’s only an adjustment at first.
Like many people who are unilaterally deaf, I have a fear of losing hearing in my good ear. It’s gotten easier over the years though and that fear doesn’t emerge often in my daily life.
Once again I appreciate you doing this study. Most people aren’t aware of unilateral deafness and the extent of coping measures that are required to function with it in day to day life.
Thank you for this article! It is the most accurate explanation of UHL that I have seen to date. I completely lost the hearing in my left ear almost a year ago. I woke up one morning and didn’t feel quite right, but when I tried to get out of bed I barely could stand on my own and became very nauseous. It took me awhile to realize that I could not hear anything out of my left ear. I finally ended up with CROS hearing aids and while they help they also hinder. It’s a relief to know so many others feel the same. I try so hard to act as though I’m fine, but I struggle every day. I stayed home from work today (working from home) because I was simply exhausted due to having family over for Easter. I made it to work yesterday, but just couldn’t today.
I have been looking for something for my manager to read so that he can have a better understanding of what I am going through. When I talk about it I feel like I am feeling sorry for myself and understate what I really am going through. I just can’t keep up with everything some days and it’s much easier for me to deal with in my quiet office here at home. I do go through bouts of depression as well. It doesn’t last long, but I am trying my best to try to come up with ways to overcome that. Again, thank you for this study. The impacts are significant, but so many believe that since we still can hear out of one ear….it’s not that big of a deal.