By Thomas A. Powers, PhD, Heike Heuermann, PhD, and Ronny Hannemann, PhD
This article reviews 10 of the most commonly asked questions regarding the fitting applications of frequency compression technology in Siemens micon, and provides guidelines designed to foster optimum implementation.
Despite technological advancements in amplification, severe-to-profound high frequency hearing loss configurations pose challenges. In many cases, the loss is severe enough to prevent audibility of important high frequency speech sounds. This significantly reduces speech understanding, especially in background noise, because a large percent of the speech sounds needed to understand communication are at 3000 Hz and above. To compound the issue, these high frequency sounds are the softest of the average speech spectrum, which means a high amount of hearing aid gain is often needed.
Clearly, restoring high frequency audibility is one of the most fundamental objectives when providing amplification for these individuals. The general goal is to provide enough gain for high frequency speech sounds to achieve audibility, which should lead to improved speech understanding. Unfortunately, for some downward-sloping hearing losses, these gain requirements are often beyond the capabilities of even the most advanced, powerful technology—or amplification in this frequency range may be counterproductive due to the cochlea pathology.
Frequency compression (FCo) provides a potential solution to these issues. FCo is a non-linear function that compresses and moves higher frequencies into a predetermined lower frequency region where better residual hearing is present, thereby increasing the probability of audibility. As a result of compression, the patient is able to detect sounds that were formerly too soft to be audible. The compressed frequency cues are moved to a new frequency destination, ultimately providing audibility, but at a different tonality than produced in the natural environment.
In the past year, Siemens has introduced the micon technology (see Powers and Beilin1). One of the many features of this new platform is frequency compression (FCo). The micon technology has generated several questions from hearing care providers (HCPs) fitting these instruments, which we address in this paper.
1) With some patients with downward-sloping hearing losses, frequency compression is automatically activated, but then with patients with similar hearing losses it is not. Why is this?
The Siemens micon approach to applying FCo during the automated First Fit software is unique. The overriding fitting goal is to provide amplification at the corresponding frequency using traditional methods. It is essential, therefore, to properly assure that frequency compression is only applied when conventional amplification is not possible.
For this reason, Siemens has adopted a rather conservative strategy, which is designed to be used only when necessary: preserve the sound quality of the output signal, and present the compressed signal to the wearer in a manner sounding as natural as possible. It’s possible, therefore, that a patient with moderately downward-sloping hearing loss might not meet the activation criteria, but a patient with a slightly more severe loss would.
2) Regarding the frequency compression activation criteria in First Fit, what sort of decision analysis is happening behind the scenes? Is the decision simply based on the degree of hearing loss?
Of course, the degree of hearing loss is a prominent determinate, but the algorithm also takes other factors into consideration. Specifically, the micon frequency compression feature is implemented based on an algorithm that considers these four different factors:
• The degree of the high frequency hearing loss;
• The prescribed gain for the high frequency region;
• The frequency-specific effective audibility for these high frequency regions; and
• The probability for cochlear dead regions.
3) How does prescribed gain enter into the decision process?
The prescribed gain provides a general guideline of whether it is possible to make a given signal audible using traditional amplification. For example, let’s take a high frequency fricative that occurs around 4000 Hz. We know that in the context of average speech, this fricative usually is around 50 dB SPL. We’ll say that our patient has a precipitous downward-sloping hearing loss, dropping to 100 dB HL at 4000 Hz. Doing some HL to SPL conversions, we can calculate that we could make a 50 dB SPL signal audible at this frequency with ~65 dB of gain. However, that would not only be considerably more than prescribed by any prescriptive fitting approach, but also unacceptable to the patient. We, therefore, can use prescribed gain as a calculation to determine if a given signal will be made audible.
We also should point out that there are three fitting algorithms within Siemens’ CONNEXX fitting software: micon fit, NAL-NL2, and DSL5. The prescriptive fitting method selected also can impact the need for FCo, as these methods do not prescribe the same amount of gain for the higher frequencies.
4) Is frequency compression always implemented when cochlear dead regions are present?
The short answer is “no,” but there is more to it. It is the general understanding that cochlear dead regions are an area in the cochlea where the inner hair cells and/or the auditory neurons are functioning very poorly, if at all. It is difficult to know exactly when they are present using routine audiologic measures, although we can predict—to some level of certainty—from the degree of loss and the configuration of the audiogram. It is also possible to use the Threshold Equalizing Noise (TEN) test to help identify potential dead regions,2,3 although the sensitivity and specificity of this test is, of course, not 100% either.
Also, the knowledge of dead regions present does not necessarily trigger the use of FCo. For example, let’s look at a downward-sloping hearing loss that drops precipitously to 70 dB at 3000 and 4000 Hz, and we know that there are dead regions at these frequencies. Moore2 suggests that we apply amplification through the frequencies that are 1.7 times the lower edge of the dead region, which in this case would be 3,000 Hz. This involves applying traditional amplification up to 5100 Hz (3000 X 1.7) for this patient. This idea is supported by the research of Cox et al,4 who showed that when high-frequency dead regions are present and hearing loss is moderate to severe, on average patients will achieve improved speech understanding when gain is provided within the dead region.
So, while we do take the potential presence of dead regions into account, the prevailing criterion for activating FCo will be if we can provide gain using traditional amplification, as discussed earlier. While many of the patients selected for FCo will have dead regions, the presence or absence of a cochlear dead region only indirectly impacts the amplification scheme.
5) Is it okay to implement frequency compression for open fittings?
There certainly are many patients who meet the high-frequency criteria for FCo and have normal hearing in the low frequencies, making them candidates for an open-canal (OC) fitting. We are not aware of research, however, which has directly examined the question regarding their candidacy for FCo.
There is the potential for a negative consequence. If the ear canal is open, direct sound will not be restricted, and will strike the eardrum at about the same time as the amplified sound. If the amplified sound has undergone FCo, it is possible that two different signals arriving at the same time may sound distorted to the patient. This will probably only occur around 1500 Hz. Below that the signal is not compressed, and above that frequency range there won’t be much direct sound audible, even with an open fitting. Also, if considerable gain is applied to the compressed signal, there may be an increased probability of acoustic feedback when FCo is applied in an OC fitting.
As mentioned earlier, since the introduction of micon FCo, the approach has been a conservative application, so we do not automatically implement FCo if it has been noted in the software that it is an open fitting. On the other hand, we don’t discourage the trial of this technology with selected patients who have OC fittings, as in many cases there probably will be a positive result. Many hearing care professionals will activate FCo in the second program and allow the patient to conduct real-world comparisons during the first few weeks of micon use.
6) How are the “correct” settings obtained for FCo when it isn’t the default setting in the software for a given hearing loss?
Even when FCo is not the default setting, calculations have been made in the CONNEXX software that provide a reasonable starting point. These calculations are applied when FCo is activated. There are two aspects to the activation of the FCo feature:
Candidacy. The candidacy rule first distinguishes between the new and the experienced user. In our studies, we have observed that new hearing aid users find it difficult to adjust to the frequency-lowered sounds (either compressed or shifted). For this reason, in the case of new users, the FCo feature is by default off, regardless of the actual hearing loss.
Parameterization. The FCo parameters are still calculated in the background on the basis of the gain estimation rule (a function of the combination of the hearing loss, generic or proprietary formula chosen, dead region estimation, and speech cues mapping), and they are applied if the FCo is switched on manually.
For the experienced users, the candidacy depends predominantly on the gain estimation rule (as described above for new users). A detailed description of how these parameters are determined can be found in a white paper by Serman and colleagues (micon Frequency Compression. Available at: www.hearing.siemens.com).
7) Is it possible to use frequency compression to solve acoustic feedback problems?
Possible, yes. Reasonable, no. As Susan Scollie, PhD, nicely stated in a recent article by Mueller et al5:
“The use of frequency-lowering to avoid feedback is, at minimum, a lazy practice because it increases the risk of decreasing speech intelligibility. There are much better ways to handle feedback issues.”5
We agree with this statement. Siemens’ instruments are equipped with a sophisticated feedback reduction system that has performed superiorly in clinical trials.6 With this system, we can maintain audibility at the frequency of feedback, unlike what would happen if FCo was employed.
8) Could you explain the frequency compression terminology that is used in the software? Some of the terms sound similar.
There are some new terms associated with the frequency compression feature. Here are the three that are most commonly used, with a brief definition of each:
• Fmin: Represents both the lower boundary of the target frequency region that needs to be compressed and the lower boundary of the compressed region. Example: If the Fmin was set to 2000 Hz, no signals below 2000 Hz would be compressed; 2000 Hz would then be the lower boundary of the compressed signals.
• Fmax: The upper boundary of the compressed region. Ideally, this should fall at or near the highest potentially audible frequency of the patient. Example: If a patient with a downward-sloping loss had thresholds going from 40 dB at 2000 Hz, 60 dB at 3000 Hz, and 100 dB at 4000 Hz, we would set Fmax slightly above 3000 Hz, as the compressed signal might not be audible at higher frequencies.
• Fratio: While not directly programmable, the FCo ratio is displayed in the CONNEXX 7 software. This ratio is based on the Fmin and Fmax settings—the smaller the range between these two settings, the larger the ratio. The frequency compression is nonlinear, and so, the ratio displayed represents the overall compression function employed.

|
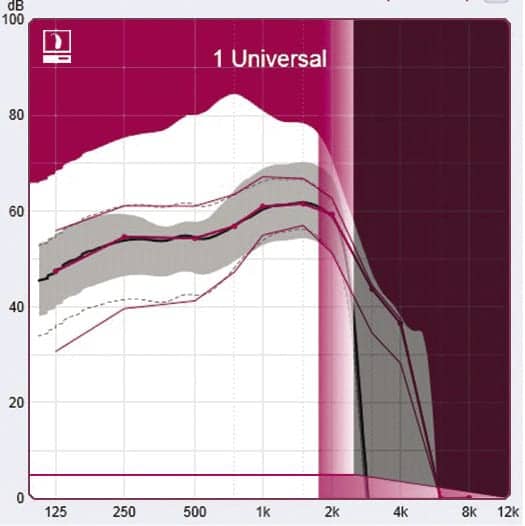
| Figure 1. CONNEXX screen shot of FCo settings. In this example, shown in shaded pink, Fmin has been set at 1700 Hz (starting point of compression) and Fmax is set to 2500 Hz (the upper destination boundary for the compressed signal). The shaded area above 2500 HZ represents the frequencies that have been lowered. |
Figure 1 is an illustration of how FCo is displayed in the CONNEXX software. Note that the destination region is shaded in pink, representing Fmin to Fmax. The grey area in the higher frequencies (Fmax to Fend) represents the region where gain is no longer applied.
9) What is the best procedure during the fitting process to determine if FCo has been set optimally for each individual patient?
The micon FCo parameters that are selected by the CONNEXX software are a good starting point. But verification on the day of the fitting is still necessary. Based on this evaluation, the degree of frequency compression may need to be stronger or weaker. Before discussing verification techniques, there are a couple of important points to remember regarding this verification and adjustment procedure:
• The gain that is applied to the frequency-compressed signals will be the same as the gain that was originally programmed for the destination frequencies. That is, if 25 dB of gain has been applied for a 55 dB SPL signal at 2000 Hz, and a 6000 Hz signal of 55 dB SPL has been compressed to the 2000 Hz signal, the 6000 Hz signal will receive 25 dB of gain. Of course, some patients—especially new users—are reluctant to use the prescribed gain. If the patient-driven fitting approach results in lowering gain, then these patients may not have enough gain to make the compressed signals audible.
• However, if the compressed signal is not audible to the patient, randomly increasing gain in the destination area may cause harsh sounds to originate at this frequency. This may result in patients turning down overall gain (if they have a VC), significantly reducing audibility for other important frequencies.
10) What specific verification methods can be used?
One procedure that helps assure the speech signal was compressed appropriately is real-ear probe microphone measures (see articles by Alexander,7 Scollie,8 and Mueller et al5). With this approach, it is possible to use speech signals or live-voice input signals to examine the ear-canal SPL compressed signal and compare this output to the patient’s hearing thresholds at key frequencies. More or less aggressive compression can then be applied accordingly.
Not all dispensing professionals have probe-mic equipment, however, and therefore a popular form of FCo verification is live-voice communication (partially because of its simplicity). This can involve talking or reading passages to the patient, or the vocalization of key high frequency speech sounds such as /s/ and /sh/. It is also important to have patients talk or read passages to determine how they perceive their own voice. Research9 with FCo has even used the phrase we all heard in childhood: “Sally sells seashells by the seashore.”
The goal of FCo is to make the compressed signal audible, reasonably acceptable, and not annoying. One wouldn’t expect it to sound “normal,” which is why we use the term acceptable. If the fitting is for a new hearing aid user, it may be that the amplified signal in general will not sound “normal” with FCo on or off. Given the degree of hearing loss recommended for FCo activation, if the aided /s/ is audible, we can assume it’s because of compression. HCPs using live-voice presentation of the /s/ and /sh/ in isolation should try not to present these sounds louder than how they occur in normal conversation—around 50-55 dB SPL.
We know that some clinicians conduct formal speech testing on the day of the fitting to determine if FCo is providing benefit. The compressed speech signal is unique. It is not likely that the benefit for speech understanding will be noticeable the day of the fitting. In fact, some research has shown that frequency lowering can initially make recognition of some syllables worse rather than better. While formal speech testing can be conducted on the day of the fitting, and used as a baseline, it is unlikely that these results will predict the benefits that may be present after weeks or months of regular hearing aid use.
Summary
Frequency compression is an intriguing new technology. It has provided benefits for a significant group of hearing-impaired individuals, but when applied inappropriately, it also can reduce speech understanding and overall sound quality.
For that reason, Siemens has adopted a conservative strategy for its implementation, which is designed to use FCo only when necessary, preserve the sound quality of the output signal, and present the compressed signal to the wearer in a way that sounds as natural as possible. The overriding fitting goal is to provide amplification at the corresponding frequency using traditional methods whenever possible. ?
References
1. Powers TA, Beilin J. True advances in hearing aid technology: What are they and where´s the proof? Hearing Review. 2013;20(1):32-39. Available at: /products/21336-true-advances-in-hearing-aid-technology-what-are-they-and-where-s-the-proof-january-2013-hearing-review
2. Moore BC. Dead regions in the cochlea: conceptual foundations, diagnosis, and clinical applications. Ear Hear. 2004;25(2):98-116.
3. Moore BCJ. Testing for cochlear dead regions: Audiometer implementation of the TEN(HL) test. Hearing Review. 2010;17(1):10-16,48. Available at: /practice-management/16935-testing-for-cochlear-dead-regions-audiometer-implementation-of-the-tenhl-test
4. Cox RM, Johnson J, Alexander G. Implications of high-frequency cochlear dead regions for fitting hearing aids to adults with mild to moderate severe hearing loss. Ear Hear. 2012;33(5):573-587.
5. Mueller HG, Alexander J, Scollie S. 20Q: Frequency lowering—the whole shebang. AudiologyOnline, Article 11913 (June 2013). Available at: http://www.audiologyonline.com/articles/20q-frequency-lowering-whole-shebang-11913
6. Chalupper J, Powers T, Steinbuss A. Combining phase cancellation, frequency shifting and acoustic fingerprint for improved feedback suppression. Hearing Review. 2011;18(1):24-29. Available at: /practice-management/17061-combining-phase-cancellation-frequency-shifting-and-acoustic-fingerprint-for-improved-feedback-suppression
7. Alexander JM. 20Q: The highs and lows of frequency lowering amplification. AudiologyOnline, Article 11772 (April 2013). Available at: http://www.audiologyonline.com/articles/20q-highs-and-lows-frequency-11772
8. Scollie S. 20Q: The ins and outs of frequency lowering amplification. AudiologyOnline, Article 11863 (May 2013). Available at: http://www.audiologyonline.com/articles/20q-ins-and-outs-frequency-11863
9. O’Brien A, Yeend I, Hartley L, Keidser G, Nyffeler M. Evaluation of frequency compression and high-frequency directionality. Hear Jour. 2010;63(8):32-37.
About the Authors:
Thomas A. Powers, PhD, is Vice President of Product Management and Government Accounts at Siemens Hearing Instruments in Piscataway, NJ, and Heike Heuermann, PhD, and Ronny Hannemann, PhD, work in the Audiology Department of Siemens Audiologische Technik in Erlangen, Germany.
CORRESPONDENCE can be addressed to Dr Powers at: [email protected]
Citation for this article: Powers TA, Heuermann H, Hannemann R. 10 questions about frequency compression. Hearing Review. 2013;10(11):20-29.
Tech Topic/October 2013 Hearing Review


