
Research | March 2014 Hearing Review
If we are to be proponents of the idea that better hearing leads to better health, then we should also recognize that a more fit body can positively impact hearing.
By Helaine M. Alessio, PhD, and Kathleen Hutchinson Marron, PhD 
Editor’s Note: This article originally appeared as Chapter 6 in the book, The Consumer Handbook on Hearing Loss & Hearing Aids: A Bridge to Healing, 4th edition, edited by Richard Carmen, AuD (Aurical Ink Publishers, 2014).1 It appears here in an abridged version with permission from the publisher. For Part 2, click here.
Noise exposure and age seem to be two main culprits associated with hearing loss. Given enough time and exposure to noise at either work or leisure, or short-term exposure to very loud noise (such as from firearms or loud music), hearing acuity is likely to decline with age. However, recent evidence has accumulated identifying factors that have little to do with age or noise exposure—yet have a significant influence on hearing acuity. Some of these factors include marital status, education, personality type, and health and fitness.
In particular, as remarkable as it may sound, cardiovascular (CV) health and fitness have been studied and found to influence hearing. CV health and fitness can be measured in a variety of ways and are often assessed in a rested and fasted state through the collection and analyses of blood for lipids. This would include cholesterol and triglyceride levels that indicate how well blood flows and delivers oxygen throughout the body.
The more cholesterol and triglycerides in the blood, the more blockages there are in blood vessels. This can result in excessive stress that can damage the heart in its effort to circulate blood and oxygen throughout the body.
Another measure of CV health and fitness includes a graded exercise test that utilizes either a stationary bicycle or treadmill. A person’s heart rate is monitored, and breathing is analyzed for oxygen consumption, then converted to units of measure (such as maximal oxygen uptake). This is represented as VO2max: the maximum amount of oxygen that a person can breathe in with their lungs, pump out with their heart, and send via blood to working muscles for energy. It represents the CV system’s ability to function at peak capacity and is considered a benchmark measure of CV health and fitness. Heart rate and the amount of oxygen you can get into your cells (VO2) can be measured when biking, walking, or running at increasing workloads until you can no longer continue due to fatigue, or until a preset target of intensity is reached. There is overwhelming evidence that regular exercise can increase VO2max by 10% to 25%, and the higher the VO2max, the lower the risk for heart disease, hearing loss, and premature death from all causes.
The overall benefit of exercise cannot be overemphasized. Figure 1 shows the association between VO2max and mortality (as measured by number of deaths in 10,000 persons). Individuals with VO2max values that were in the low-fit category (below 31 ml/kg/minute for women and below 34 ml/kg/minute for men) were at higher risk for metabolic and cardiovascular diseases including obesity, diabetes, and stroke. Those with VO2max values greater than 31 ml/kg/minute for women, and greater than 34 ml/kg/minute for men, benefited by reducing those metabolic and cardiovascular risk factors and also having better hearing acuity.
The Why, When, and How for Getting Your Health and Hearing Evaluated
Why. Former Secretary-General of the United Nations Kofi Annan is quoted as having said, “Knowledge is power. Information is liberating.” Not knowing one’s health risk status may, on the one hand, contribute to a stress-free state of mind. On the other hand, the reality of one’s health risks eventually reveals itself—often in premature diseases that could be avoided or mitigated with appropriate and timely intervention.
A special category of diseases called “Silent Diseases” are described as those that produce minimal or no symptoms, although, if left untreated, may result in severe, life-changing, or even fatal consequences. The most important of these is heart disease. Risk factors include hypertension, smoking, sedentary lifestyle, obesity, and high cholesterol and triglycerides—all of which can be measured.
You can start a health-promoting intervention likely to include lifestyle change, stress management, and/or in many cases pharmaceutical intervention by:
- Assessing blood pressure;
- Quantifying the number of cigarettes smoked on a daily basis;
- Measuring the number of steps taken per day or time (in minutes) spent in physical activity;
- Measuring or predicting VO2max;
- Assessing body composition; and
- Knowing your blood lipid profile.
In some cases, surgical intervention (eg, angioplasty, gastric bypass, coronary artery bypass) is necessary, especially in cases where a silent disease is left unchecked for too long and damage has occurred in the heart or blood vessels. Those with metabolic disorders are also at risk. Once damage is repaired, however, most patients who had a variety of CV conditions, including blocked arteries and congestive heart failure among others, can return to normal productive lives.
When. So, if knowledge is power and information is liberating, then it’s important that assessment of cardiovascular health and hearing occurs early and often. How early and how often? Answers to these questions depend on many factors including the typical health and hearing screenings that occur at schools, in annual medical visits often designated as preventive or wellness visits, or at diagnostic health visits. These procedures are initiated as a result of problems perceived by individuals themselves, or by family members, friends, or teachers who notice signs and symptoms of health or hearing deficits.
How. Typical health evaluations include an assessment of health risk based on physical, mental, and social health. Regular health and wellness visits begin shortly after birth. By the time individuals reach school age, regular annual visits are expected and even required for enrollment by many school systems. After high school, annual health and wellness visits are typically done on a voluntary basis, although some occupations may require them. Tracking height, weight, body composition, blood pressure, blood lipids, blood glucose, sight, hearing, reflexes, and results of a physical examination are all part of a comprehensive wellness visit.
Furthermore, information about behaviors that affect health, such as smoking, medications, drugs, alcohol, stress, and social support, among others, provides valuable information about your health status and measures your health risk. These assessments are typically performed by a medical professional such as a physician, nurse, or chiropractor. Some tests come and go, depending on cost and evidence-based research that supports their value and their association with life-threatening diseases. The American Heart Association recommends tests for blood pressure, blood lipids, blood glucose, height, weight, and specific health behaviors (especially smoking and alcohol) be performed on individuals age 20 years and older at least every 2 years.
Health and hearing assessments provide knowledge about one’s functional health status. This information can be useful for disease prediction. This knowledge also can serve as a powerful motivator to maintain or change certain behaviors that may range from subtle adjustments in diet, exercise, or noise exposure, to more extreme interventions. One such example is the decision by celebrity Angelina Jolie in 2013 to undergo a double mastectomy when she learned she carried mutations in critical breast cancer genes.
Information about one’s relative risk and functional capabilities can be affirming or alarming. However, in either case, it also can be liberating. Whether one agrees or disagrees with Angelina Jolie’s decision, a major issue is that knowledge she received from her healthcare provider motivated her to choose a course of action to address her specific health risk. Once you have and understand information about your health and hearing status, then you’re free to make choices that are appropriate for your unique situation.
Inaction or inappropriate action may cause a minor health or hearing condition to unravel to a serious life quality issue or life-threatening condition.
Annual CV health assessments are recommended for all healthy people and typically include assessment of:
- Blood pressure;
- Body weight and height;
- Blood lipids;
- A physical exam;
- Breast or prostate examination; and
- Other tests specific to a person’s family and personal health risk, depending on age.
The US Preventive Services Task Force did not endorse a recommendation for annual hearing screening for asymptomatic adults age 50 years and older because of lack of evidence in the balance of benefits and harm.2 The Task Force did, however, recommend that adults age 50 and older who perceived hearing problems be assessed for objective hearing impairment and, when indicated by signs and symptoms, be treated appropriately.
Exercise Is Medicine for Health and Hearing
When an intervention is required to prevent further deterioration of the cardiovascular system, improve its function, or assist in recovery from an invasive surgical operation, one intriguing intervention has proven particularly beneficial. This intervention has been shown to have a dose-response effect that mimics (and in some cases exceeds) the effects of traditional medicine, with little to no side effects.
The intervention is exercise!
Decades of research investigating the benefits and risks of regular exercise have provided overwhelming scientific evidence demonstrating that, in most adults, the beneficial effects of exercise far outweigh any risks, including sudden death and acute injuries. Conclusions from exercise research include case studies to clinical trials, and have resulted in a general recommendation that a program of regular exercise should include cardiorespiratory, resistance, flexibility, and neuromotor exercise training beyond activities of daily living. Regular exercise is necessary to improve and maintain physical fitness and health and is essential for most adults.
This knowledge is gradually moving from the scientific arena to clinical settings where personal physicians are sitting down with their patients and asking them about their exercise habits. When patients share that they are sedentary (about 25% are) and admit that they don’t achieve a minimal amount of daily activity, physicians often recommend a course of action to change them from a couch potato to a physically active lifestyle.
Recommended programs
Understanding the correct intensity and duration of exercise is critical to understanding the role of exercise as medicine. And exercise is medicine! A new initiative from the largest sports medicine and exercise science organization in the world (the American College of Sports Medicine, or ACSM), along with the American Heart Association and the American Academy of Family Physicians, is in fact called Exercise Is Medicine™. A goal of this campaign is to start discussions between healthcare providers and every American to ensure that exercise is front and center in every discussion on disease prevention and wellness. The belief that exercise and physical activity are integral to the prevention and treatment of many types of health conditions is becoming accepted knowledge.
The SilverSneakers™ Fitness Program is offered by leading Medicare health plans and Medicare Supplement carriers throughout the country (including Puerto Rico). More research indicates that physical inactivity is currently the biggest public health problem in this country; the benefits of regular exercise and enhanced physical activity are not limited to heart, lungs, and skeletal muscle, but also may include organs and tissues, such as the brain, liver, pancreas, and those in the inner ear.3
Specific explanations of exercise frequency, intensity, type, and time—also referred to as the FITT principle—have been provided as a result of hundreds if not thousands of studies comparing a variety of exercise programs. Data from these comparative studies have resulted in the ACSM presenting the following evidence-based guidelines for exercise:
- Most adults should engage in moderate intensity cardiorespiratory exercise training for equal to or greater than [?] 30 minutes per day ?5 days per week for a total of ?150 minutes per week.
- Most adults should engage in vigorous intensity cardiorespiratory exercise training for ?20 minutes per day on ?3 days per week (?75 minutes per week).
- Or they should engage in a combination of moderate and vigorous intensity exercise to achieve a total energy expenditure of ?500-1000 MET minutes per week (explained next).
METS (or metabolic equivalents) are units of energy expenditure. One MET is the energy expended at rest. Three METS is the energy expended during brisk walking at approximately 3 miles per hour (mph). If a person walks at 3 mph for 30 minutes, this is equivalent to 3 METS x 30 minutes = 90 MET minutes. Six days per week of this type of physical activity would meet ACSM’s recommended energy expenditure of ?500-1000 MET minutes per week.
On 2-3 days per week, adults also should perform resistance exercises for each of the major muscle groups, and neuromotor exercise involving balance, agility, and coordination. Flexibility exercises for each of the major muscle-tendon groups (a total of 60 seconds per exercise) on ?2 days per week are also recommended.4
Impact on hearing health
Of all the types of exercises that ACSM recommends, improvements in CV health and caloric energy expenditure that result in healthier body compositions (exercises that change the body shape) are the only proven mechanisms associated with exercise that positively impact hearing sensitivity. Improvements in muscle strength and flexibility, balance, agility, and coordination have not been shown to benefit hearing.
Relationship Between Exercise, CV Health, and Hearing
Although CV health and fitness are known to have a genetic component, most research indicates that at least half of one’s CV health and fitness is determined by lifestyle and environment, and is therefore controllable to a large extent. Exercising to music from external speakers or headsets gained popularity in the 1970s and 1980s as many people actively responded to the positive news about exercise and CV health. They participated in exercise classes and moved to the music of a variety of genres and loudness. Exercise workout tapes evolved into portable MP3 players, providing even more flexibility for exercising while listening to one’s favorite tunes virtually anywhere.
Can exertion make you more vulnerable to noise?
In the midst of these popular music workouts that gained a large following in the 1980s, audiologist Richard Navarro, PhD, warned that listening to loud music while exercising might exacerbate the risk of hearing loss because of the exercise-induced redistribution of blood from the inner ear to the working muscles, leaving organs and tissues in the inner ear vulnerable to low oxygen levels.5 His hypothesis initiated experiments, a few supporting the notion that any type of stress that increased heart rate dramatically (such as exercise), regardless of whether it included noise, contributed to temporary hearing loss. One of the first studies to investigate the association between hearing sensitivity and exercise found that, when an acute bout of exercise was accompanied by noise exposure, a greater amount of temporary hearing loss occurred (compared against a resting state while in the presence of noise).6
The conclusion that one exercise session accompanied by noise resulted in hearing loss was not supported by follow-up experiments.
The first published study that investigated regular exercise and hearing acuity was conducted by Ismail and colleagues in 1973.7 They reported improved hearing in subjects who participated in an unstructured exercise program for 20 weeks. Given these conflicting results, we challenged Navarro’s theory as well as the few studies that appeared to support his work. When we conducted experiments that carefully controlled for exercise intensity, fitness level, and specific noise exposure for a set time, our laboratory could not replicate his early results. In fact, we found that one bout of exercise alone did not alter hearing. Only when subjects were exposed to high-level noise, regardless whether they were sitting or exercising, were changes in hearing observed. Furthermore, like Ismail’s study, we found that people who exercised regularly had better hearing than those who were sedentary.
Why exercise positively impacts hearing status
Over the past 30 years, it has become clear that CV health and fitness positively impact hearing. Results from different laboratories across the country have shown that, compared to low-fit individuals, people with high CV health and fitness (particularly after age 50) maintain better hearing well into old age.7-12
As researchers began to understand the role of sensory receptors in the nerve responsible for hearing, the relationship between the CV system and hearing ability became an increasingly popular topic. Exercise is positively correlated with improved blood circulation, prevention of neurotransmitter loss, and less noise-induced hearing loss.13
These changes in the vascular system allow improved blood circulation into different parts of the ear including the stria vascularis in the cochlea. This is important because the stria vascularis relies on adequate blood flow to function properly. Without constant replenishment of blood flow to the sensory receptors in the nerve of hearing, hearing ability could be compromised.
Cardiovascular fitness also may help to preserve the way in which the central nervous system interprets speech (ie, central auditory processing). It has been found that CV fitness may reduce neurotransmitter loss associated with aging and thus preserve central auditory processing.14
More studies on fitness and hearing acuity
Most certainly, the steady accumulation of scientific knowledge about the processes that protect hearing is the basis for developing successful treatments. We reported the positive effects of fitness on hearing with acute exercise and CV changes in 1994,9 and also summarized these findings in The Hearing Review.15 The study divided 28 healthy volunteers (average age 26) into three groups based on their fitness levels—high, moderate, and low. All participants had normal hearing when the study began. The researchers exposed each group to three different noise levels that are similar to what one experiences in daily life (like traffic, power mowers, vacuum cleaners, noisy toys, and amplified music). Hearing was reevaluated under three different conditions:
- After 10 minutes of noise;
- After vigorously riding a stationary bike for 10 minutes without noise; and
- After listening to noise and exercising on the stationary bike at the same time.
During all three conditions, researchers also monitored heart rate, blood pressure, and core body temperature. The high-fit group consistently demonstrated better hearing levels in all cases as compared to the low-fit group. Hearing levels for the moderately fit group fell right in the middle. Exposure to various noise levels produced more temporary hearing loss in the low-fit group than in the other two groups. The findings suggest that moderate and high levels of CV fitness may protect against hearing loss. Low-fit individuals showed the poorest hearing acuity of all groups.
It is believed that regular exercise reduces susceptibility to temporary threshold shift referred to as TTS (poorer hearing) by increasing blood flow and oxygen delivery throughout the body, including the ear. Regardless of whether it’s caused by micro- or macro-vascular pathology, insufficient cochlear blood supply can disrupt the chemical balance of the inner ear fluid (endolymph) that in turn affects the electrical activity of the hair cells and, subsequently, activation of the auditory nerve.
By improving circulation of oxygenated blood, the cochlea is less susceptible to the onset of vasoconstriction (narrowing of veins and arteries) brought on by loud noise. Regular exercise keeps blood supply and oxygen flowing at optimal levels to cells and auditory nerve fibers in the ear. Noise, not acute exercise, was responsible for causing temporary hearing loss at virtually all frequencies between 2000 Hz and 8000 Hz.
While evidence from multiple studies got exercise off the hook for causing hearing loss, further inquiry resulted in an unexpected finding. Subjects with very healthy CV fitness levels (as evidenced by high VO2max values for their age) also had the best hearing levels at nearly every frequency.9 Remember our discussion about VO2max is: the maximum amount of oxygen that a person can breathe in with their lungs, pump out with their heart, and send via blood to their working muscles for energy requirements during a maximal physical effort.
The ability to improve hearing with a CV fitness program that followed the FITT (frequency, intensity, type, and time) principle also was investigated by the authors.15 Aerobic simply means requiring air. The goal of aerobic exercise is to condition the heart and lungs to increase oxygen intake, and transport it for use by the body. In this study, subjects exercised at 70% of their aerobic capacity for 30 minutes, 3 days per week for 2 months. Ideally, we all should be getting this minimum exercise every week. It is important to understand that it’s not required to break a sweat in order to undertake an aerobic exercise. An increase of 15-25% in VO2max in these subjects (which moved them from a low-fit category to a moderate-fit category) correlated with improved hearing with the most improvement occurring at 2000 and 4000 Hz.
This led to the conclusion that regular, moderate intensity exercise resulted in improved CV health and fitness and enhanced hearing as well. Additional benefits derived were improved reflex reactions and better ability to read newsprint without eyeglasses for some subjects. These results demonstrate the plasticity of hearing acuity, as well as the CV system; that is, the ability of both systems to change for the better as a result of a positive lifestyle intervention, regardless of age.
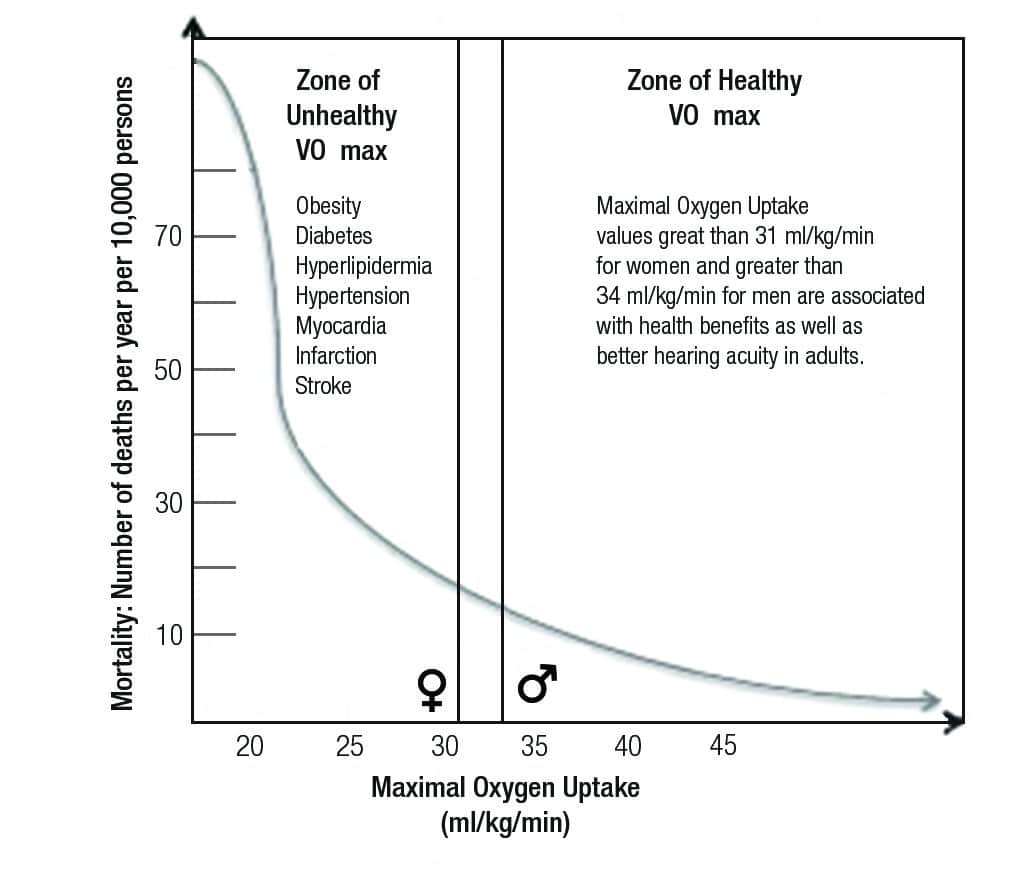
Figure 1. Association between VO2max and mortality.
Heat shock proteins and hearing loss
What may also be important is the production of heat shock proteins. Scientists believe these substances help minimize damage throughout the body. Research in cellular mechanisms in the cochlea reveals that cells under stress from noise, ototoxic drugs, and aging generate these proteins to protect surviving cells.
Several laboratories have demonstrated positive protective pharmacological effects of specific proteins against cochlear damage.16 The cochlea contains 17,500 to 23,500 hair follicles referred to as sensory hair cells. The observations that hair cells contain specific proteins that undergo changes in structure with slight swelling suggest that active elements exist to protect tissue from damage. Such proteins also may play key roles in protecting hair cells from metabolic and aging changes. Also, antioxidant research has allowed scientists to better understand the effects of certain nutrients on circulation within the ear. Results of one study using folic acid (which scavenges free radical molecules) demonstrated that participants who supplemented their diet with this protein for 3 years evidenced improvement in low-frequency hearing.17 There is evidence that people who are more fit have more of these heat shock proteins that in turn could explain how regular exercise may help protect hearing from everyday noise damage.

Figure 2. The higher the cardiovascular fitness (shown as low, medium, and high), the better the hearing acuity in most age groups.
Different fitness levels lead to different levels of hearing acuity
In another study, improved hearing was observed in older adults with high cardiovascular health and fitness; however, a surprising finding defined specific types of fitness associated with gains and losses in hearing acuity. Adults who had high muscle strength but low CV health had poorer hearing.18 Based on these results of a cross-sampling of individuals, we recommend that CV exercise be included either alone or in conjunction with strength training as a contributor to preserve and possibly enhance hearing in adults of varying ages. People in their 20s, 30s, and 40s maintained good general hearing ability, regardless of fitness level (Figure 2).
However, after age 50, people with medium and high CV fitness consistently showed better hearing at high frequencies than people of the same age with low CV fitness.
After the association between hearing, age, and CV fitness was established, we then conducted a longitudinal study of 25 people between the ages of 12 and 76 tested twice over a 5-year period.14 Our goal was to determine if CV fitness and hearing acuity changed in a similar way over time. That is, we wanted to observe if young low-fit individuals demonstrated poorer hearing 5 years later, and if young, moderate- or high-fit individuals demonstrated better hearing 5 years later. Unlike a cross-sectional study, a longitudinal study follows the same subjects for a period of time and controls factors related to historical events or actions that may affect one group of people in a particular age group, but not another (eg, different noise exposure levels in work settings).
Study participants were sorted into three CV fitness groups: high, medium, and low, and we looked at two test periods 5 years apart utilizing hearing thresholds and otoacoustic emissions. Our results showed that, unlike low-fit people whose hearing got worse 5 years later, people with high CV fitness maintained their hearing from the prior 5 years. This indicated that, at the second testing, sound did not have to be any louder in order for them to hear it than it did when they were first tested. This is a notable and desirable maintenance of hearing sensitivity over time. Furthermore, individuals with high CV fitness during the first test session who maintained their CV fitness over the 5 years between testing had better hearing acuity over time than those who did not maintain CV fitness or who had low CV.
…And poor fitness leads to poorer hearing acuity
An important conclusion from virtually all of these experiments is not just that high cardiovascular fitness is correlated with better hearing sensitivity, but also that adults with the lowest level of CV fitness virtually always had poorer hearing. This was also evident when considering an individual’s age and gender, indicating that CV fitness has a protective effect on hearing as a person ages.
The relationship between CV fitness and hearing was confirmed in a national study on hearing sensitivity using data collected from the 1999-2004 National Health and Nutrition Examination Survey. The study included 1,082 participants representative of 42,869,850 adults between the ages of 20 and 49. It found that, compared to low-fit individuals, males as well as females with good hearing had higher VO2max values.13 The correlation between exercise and hearing was particularly strong for female participants. These females with high cardiovascular fitness levels also were found to have better hearing at lower frequencies as well as higher frequencies. These findings indicate that cardiovascular health is a powerful influence over hearing sensitivity, and individuals with high CV fitness can maintain better hearing acuity well into adulthood, while persons with low CV fitness are likely to have poorer hearing.
Part 2 of this article looks at body composition and hearing, as well as factors that influence hearing status other than noise.
References
1. Alessio HM, Hutchinson Marron K. Fitness and better hearing. In: Carmen RE, ed. The Consumer Handbook on Hearing Loss & Hearing Aids: A Bridge to Healing. 4th ed. Sedona, Ariz: Aurical Ink Publishers; 2014. Available at: http://www.hearingproblems.com
2. Moyer VA. Screening for hearing loss in older adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:655-661.
3. Blair SN. Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med. 2009;43:1-2.
4. Garber CE, Blissmer B, Deschennes MR, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334-59.
5. Navarro R. Sports scan. Physician Sports Med. 1990;18:6.
6. Saxon SA, Dahle AJ. Auditory threshold variations during periods of induced high and low heart rates. Psychophysiol. 1971;8:23-29.
7. Ismail AH, Corrigan DL, MacLeod DF, et al. Biophysiological and audiological variables in adults. Arch Otolaryngol. 1973;97:447-451.
8. Alessio HM, Hutchinson KM. Effects of submaximal exercise and noise exposure on hearing loss. Res Q Exerc Sport. 1991;62:413-419.
9. Manson J, Alessio HM, Cristell M. Does cardiovascular health mediate hearing ability? Med Sci Sports Exerc. 1994;26:866-871.
10. Kolkhorst FW, Smaldino JJ, Wolf SC, et al. Influence of fitness on susceptibility to noise-induced temporary threshold shift. Med Sci Sports Exerc. 1998;30:289-293.
11. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults: data from the National Health and Nutrition Examination Survey, 1999-2004. Arch Intern Med. 2008;168:1522-1530.
12. Hutchinson KM, Alessio HM, Baiduc RR. Association between cardiovascular health and hearing function: pure-tone and distortion product otoacoustic emission measures. Am J Audiol. 2010;19:26-35.
13. Hull RH, Kerschen SR. The influence of cardiovascular health on peripheral and central auditory function in adults. Am J Audiol. 2010;19:9-16.
14. Cristell M, Hutchinson KM, Alessio HM. Effects of exercise training on hearing ability. Scand Audiol. 1998;27:219-224.
15. Alessio HM, Hutchinson KM. Exercise promotes hearing health. Hearing Review. 2004;11(4):36-37.https://hearingreview.com/all-news/15862-exercise-promotes-hearing-health
16. Taleb M, Brandon CS, Lee FS, et al. Hsp70 inhibits aminoglycoside-induced hearing loss and cochlear hair cell death. Cell Stress Chaperones. 2009;14:427-437.
17. Durga J, Verhoef P, Anteunis LJ, et al. Effects of folic acid supplementation on hearing in older adults. Ann Intern Med. 2007;146:1-9.
18. Hutchinson KM, Alessio HM, Hoppes S, et al. Effects of cardiovascular fitness and muscle strength on hearing sensitivity. J Strength Cond Res. 2000;14:302-309.
Original citation for this article: Alessio H, Hutchinson K. Fitness and better hearing, Part 1. Hearing Review. 2014;21(3): 18-24.



