Tech Topic | February 2020 Hearing Review
By Laura Winther Balling, PhD; Niels Søgaard Jensen, MSc; Oliver Townend, and Wendy Switalski, AuD, MBA
A much-used quote relating to the use (or misuse) of statistics is: “It’s very possible for a man to drown standing in a river that has an average depth of 6 inches.” In other words, averages do not always reflect practical experience. This holds for many things, including hearing aid fittings.
How many times have you heard someone say or read a post on a listserv that says: “I just fit a patient to [NAL-NL2, DSL5.0, or manufacturer’s first fit], and the patient said he didn’t like it. These fitting algorithms don’t work,” or “This hearing aid from [manufacturer] is supposed to have a great program for listening in background noise, but my last patient didn’t like it at all. I’m going to try a different manufacturer.” Even when best practices are followed in the fitting process and the best technology is used, it is probable (not just possible, but probable) that approximately one-third of hearing aid wearers will not be immediately pleased with the initial fitting. The reasons for this will be discussed, prior to providing a unique solution.
Why Targets Are Fallible
Preferred loudness. An essential ingredient of prescriptive hearing aid fittings is determining frequency-specific gain, the calculation of which is based primarily on the average preferred gain for someone with a specific degree of pure-tone hearing loss. Whether viewing the manufacturer’s fitting screen or doing probe-mic verification, we see a plot of these target values. When conducting real-ear verification, it is common practice to adjust gain until output matches these targets. It is important to remember, however, that although the “target” looks like a single dB value, it is in fact a range. Keidser & Dillon1 reported on preferred gain levels as part of the data they collected for the development of the NAL-NL2. They show preferred gain for average inputs across varied levels of average hearing loss (n=189 experienced hearing aid users). They report a range of ~12-15 dB in preferred gain level for all common hearing loss levels. If we assume that average was the middle of this range, which would then determine the prescriptive fitting target, we could expect user preferences to vary from target by ±6 dB, or even more.
Loudness discomfort levels (LDLs). While conducting frequency-specific loudness discomfort levels for each hearing aid wearer is generally recommended by best-practice documents,2 most hearing care professionals (HCPs) either intentionally or unintentionally use default average values. Bentler and Cooley 3 looked at the variability of LDLs and reported average LDL values from 710 individual ears. For a hearing loss of 50 dB HL, the average LDL was 102 dB SPL (re: 2cc coupler, around 100 dB HL). However, the range was from 72 to 130 dB SPL. The authors also reported that only one-third of the participants were within ±5 dB of the average.
The most obvious impact of this is that the programmed gain for loud inputs could be significantly too soft or too loud for many hearing aid users. However, the LDL also has an impact on preferred gain for average inputs, as this is typically influenced by the measured or predicted residual dynamic range (LDL minus the hearing threshold). The outcome is that what appears to be a perfect fit to target on the fitting screen using average LDLs could easily be off by 5 dB or more when the hearing aid user’s true measured LDLs are applied to the fitting process.
Real-world experiences. Hearing aids are fitted in a relatively sterile environment. Additionally, the fitting itself is centered around the predicted real-world listening experiences of the average hearing aid user. Compromises are required to balance listening in quiet and listening in noise; sound quality and speech intelligibility; focused listening and relaxed listening. However, each individual user is unique in their real-world listening needs and experiences, and averages are unlikely to cover all these needs and experiences.
Listening intention. Another challenge relating to the use of “average” fitting values concerns the automatic signal processing of hearing aids, steered by the signal classification system. The automatic steering is based on what is assumed to be of interest in a specific environment. A talker that is 10 dB louder than others leads the classification system to assume that that is what the hearing aid wearer wants to focus on—and in many cases this will be true. However, even the best automatic classification system will not know the intention for each specific user in a specific sound environment. For example, a dominant talker in a noisy restaurant may lead the automatic processing scheme to focus on this talker, on the assumption that this is the listener’s primary signal of interest. In reality, the listener’s intention might be quite different. For example, they may be more interested in relaxing at the table next to the dominant speaker or in focusing on a different speaker.
A Solution for the Challenges of “Average”
It is clear that using average values will not always lead to the best hearing aid outcome. At first consideration, giving the hearing user a way to control gain may appear to solve this problem; however, this is not the case, for several reasons. First, it is unlikely that the difference from average is equal across frequencies. Second, regarding preferred loudness, the programmed loudness level is often adequate for one or more input levels (eg, soft inputs), but not for other inputs—so changing gain to fix one problem may create a new problem. Finally, even if changing gain worked, the wearer would then have to change gain every time they experienced that specific listening situation.
Some of the problems reviewed here can —and should—be solved by fine-tuning of the hearing aids by the HCP. However, solving all the problems would require the hearing aid user to visit the clinic far more often than what is feasible and also to clearly define their challenges, including the exact listening situation and their precise listening preferences in that situation, which is an impossibility for most users. The obvious solution is that changes need to be made by the user in real time during the listening experience. That is exactly what can be accomplished with SoundSense Learn.
Widex SoundSense Learn (SSL) is an implementation of a well-researched AI approach, designed to individualize hearing aid parameters by sampling enough possible settings to adjust the hearing aids according to the user’s preference for a given listening situation.4 SSL varies gain settings in three frequency bands based on user input through their smartphone app. Through a machine-learning approach, optimization can be obtained quickly through an A/B paired-comparison methodology. This allows the hearing aid user to listen to two sets of parameters and indicate their relative preference. Their selection determines the next parameter settings to be compared, and within a few comparisons the optimum setting is achieved.
The result is a personalized setting that can be used just for that moment or saved as a program for later repeat use. In the first place, the SSL settings are only applied in the given SSL program, but, as described below, they may be used by the HCP as a basis for more general fine-tuning.
The A/B comparison approach is crucial in this optimization procedure. Auditory sensory memory (precise memory of sound after it vanishes) is very short—only a few seconds. This is a problem for typical clinical comparisons of different hearing aid programming, as by the time the listeners hear the second sound sample, they no longer have a vivid memory of the first. By contrast, this challenge is eliminated with the rapid A/B comparisons used in SSL.
The advantages of SSL include:
- Settings can easily be personalized to the user’s preferences in different real-world listening situations.
- Settings can be customized whenever listening intention changes.
- Preferred settings can be saved for future use.
- Users are likely to take greater ownership of the fitting process, which will lead to increased benefit and satisfaction.
- Unscheduled repeat visits to the HCP may be reduced, as minor fitting issues can be solved by the user.
- The HCP can use the adjustments made by users with SSL for more global fine-tuning, using the Real-Life Insights feature in Compass GPS.
Research Evidence Supporting SoundSense Learn
Since the introduction of SSL, several studies have been conducted in both the laboratory and the real world to evaluate the effectiveness of this approach.
Townend et al5 conducted a study to determine if SSL would result in improvements for different sound scenarios and listening intentions when the resulting setting was compared to the initial setting (the prescribed Universal program with all adaptive features turned on). Atotal of 19 individuals with mild-to-moderate hearing losses listened to different auditory environments processed by Widex EVOKE test hearing aids and used the SSL application to manipulate hearing aid settings. The participants were given visual context and written instructions to guide their auditory intention towards a given sound attribute (eg, listening comfort or sound quality). Recordings of all the processed auditory environments, using both the Universal and SSL-adjusted settings of the hearing aids, were then made. Upon their return visits, they rated the sound attribute associated with the given environment for each recording.
The participants rated listening comfort in three different sound environments and showed a significant increase in listening comfort for the SSL setting, with the results shown in Figure 1 (p<0.01). The participants also rated the overall sound quality of three different pieces of music. Comparative testing showed a significant increase in reported sound quality with SSL (p<0.05; see Figure 1).
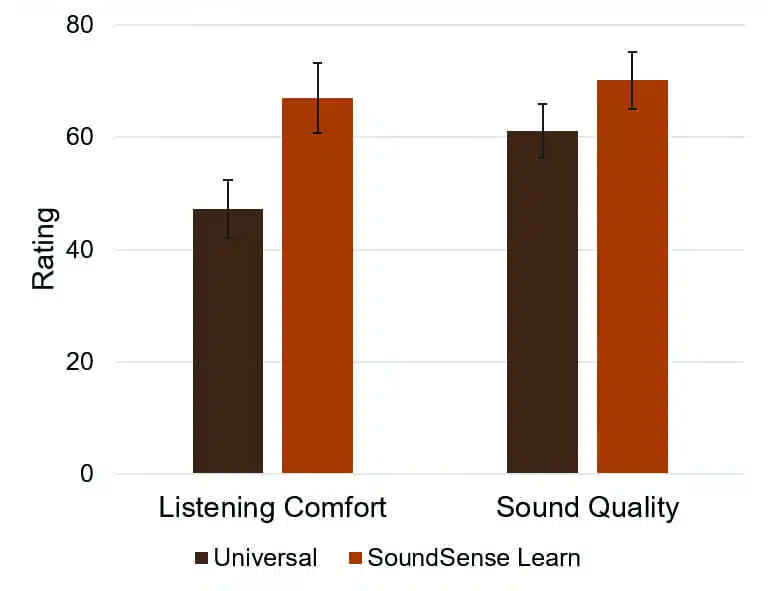
These laboratory findings clearly revealed that SSL can improve both listening comfort and sound quality, and comparable results were found in a similar study conducted at another test site.6
The next step was to examine if these benefits would carry over to the use of SSL in the everyday life. To evaluate the real-world effectiveness of SSL, it was included in a large-scale study of hearing aid users.7 The user survey was conducted across nine different countries, involving a total of 118 experienced hearing aid users who were fitted with Widex EVOKE 440 Fusion2 hearing aids.
Of the 118 individuals surveyed, 53 (44%) reported that they used SSL during their first few weeks of hearing aid use. Their impression of SSL was very positive: 38 (72%) reported it helped improve specific listening situations, and 42 (80%) stated that they would recommend the use of SSL to others.
The data above reveals that 56% of the hearing aid users in the survey did not use SSL. This is an expected finding which takes us back to our discussion of “average.” We would expect that about two-thirds of hearing aid users would fall close to average, and therefore the programmed gain and output of the initial fitting would be appropriate. For these individuals, EVOKE’s powerful automation will provide the needed audibility, sound quality, and noise reduction, making further adjustments unnecessary.
In addition to data from studies and surveys, SSL usage also generates large amounts of anonymous data that can serve as input to hearing aid development and help us understand the real-life hearing of SSL users. This is an excellent example of how real-life data—and smart use of that data—can really advance a field, in this case hearing aids.
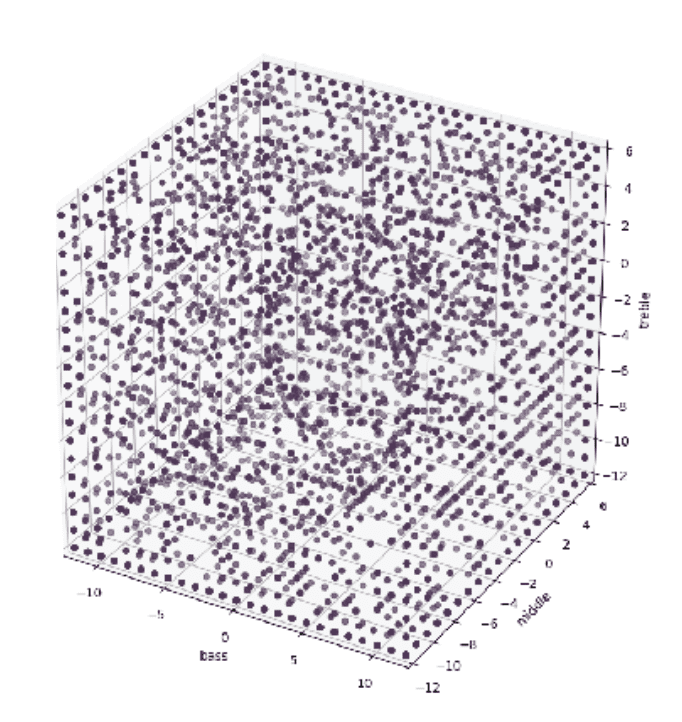
We will focus here on two aspects, based on a sample of 13,813 unique programs created by 5,448 unique end users in studies published in 2019.8,9 First, it is interesting to explore which gain adjustments users make. For example, if all the adjustments of the low frequency band are made in a certain direction, we could conclude that this was related to the fitting rationale. However, this is clearly not the case, as seen in Figure 2 where each program is plotted as a dot in 3-dimensional space depending on the adjustments made in the bass, middle, and treble frequency bands. The personalized programs are distributed throughout the three-dimensional space, with no clusters. This indicates that the personal programs created with SSL are indeed highly personal. From a practical perspective, each dot represents a potential need for fine-tuning that did not require a visit to the clinic because the user had access to SSL.
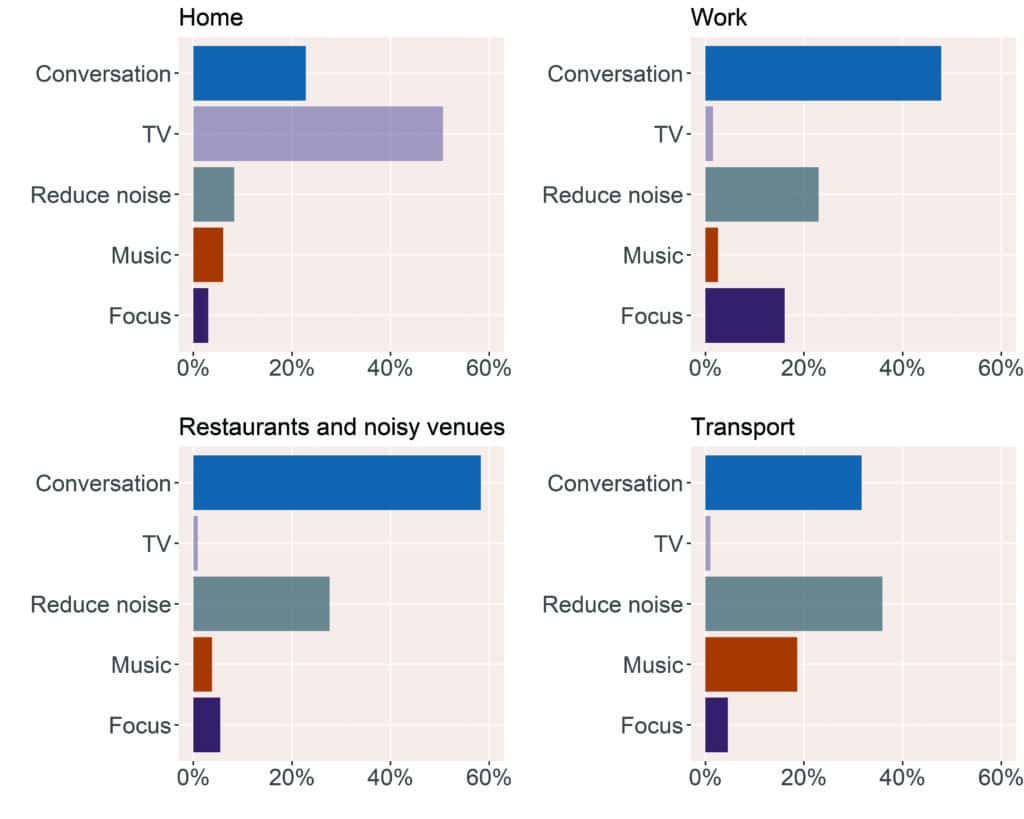
Next, we are interested in understanding the situations and auditory intentions for which SSL is used. Every time a new SSL program is created, the user is asked to indicate the situation and their intention. These data can be explored in various ways, and Figure 3 shows the relative frequencies of the top-5 intentions in four different categories of situations: 1)home; 2) work; 3) restaurants and noisy venues, and 4) transport). We see that the frequency of these intentions varies between situations. For example, the balance between conversation and noise reduction varies substantially, with conversation being most important in restaurants and noisy venues, while noise reduction is more important during transport. This further supports the need for personalization based on intention in the moment. Moreover, this information on situation and intention is provided to the HCP through the Real-Life Insights functionality in Compass GPS, which we discuss next.
SoundSense Learn and Counseling
Real-Life Insights (RLI), incorporated into Compass GPS, provides the HCP with insights about the individual hearing aid users and their hearing needs and preferences in real life. Through RLI, the HCP can (with the user’s consent) examine the SSL programs the user has created, including both the selected settings and the use patterns. When trends are noted across the personal programs, these can be used for more general adjustments of the hearing aid settings. This helps solve the “average” problem more generally by allowing the HCP to make meaningful changes in programming, based on situation-specific data collected by the user, without the need for very precise descriptions of situations and perceptual listening experiences, which we know are difficult to obtain. In addition to this, RLI gives the HCP insights into the real-life hearing of their patients and a well-informed basis for counselling.
Summary
Not everyone is “average.” This can cause the initial hearing aid fitting to be less than optimal for many users. The Widex fitting approach takes several steps to individualize the fitting thoroughly from the very beginning by using experienced vs inexperienced fitting profiles, accounting for individual ear acoustics by using the Sensogram, and using advanced vent compensation corrections.10
Despite this detailed fitting approach, for some hearing aid users, changes will still be desired, partly due to listening intentions that vary depending on the situation. When this occurs, SSL clearly provides a solution. Research shows it is easy to use, and it improves performance in the majority of cases, across intentions. The ability for the wearer to “fix the problem” in the moment provides immediate satisfaction, empowers the wearer in daily life, and may reduce office visits for fine-tuning — a benefit for both the hearing aid user and the HCP. Moreover, the user’s personal programs shown in RLI in the Compass GPS software offer useful information for the HCP when fine-tuning is needed. These advanced tools offer a solution for all users—so not being “average” is no longer a problem.
CORRESPONDENCE can be addressed to Dr Balling at: [email protected]
Citation for this article: Balling LW, Jensen NS, Townend O, Switalski W. SoundSense Learn: When average is not enough. Hearing Review. 2020;27(2):30-33.
References
1. Keidser G, Dillon H. What’s new in prescriptive fittings down under? In: Proceedings from the Phonak Hearing Care for Adults Conference; November 13-15, 2006; Chicago, IL.
2. Valente M, Abrams H, Benson D, et al. Guideline for the audiologic management of adult hearing impairment. Audiology Online. https://www.audiologyonline.com/articles/guideline-for-audiologic-management-adult-966. October 30, 2006.
3. Bentler RA, Cooley LJ. An examination of several characteristics that affect the prediction of OSPL90 in hearing aids. Ear Hear. 2001;22(1):58-64.
4. Nielsen JBB, Nielsen J, Larsen J. Perception-based personalization of hearing aids using Gaussian processes and active learning. IEEE/ACM Transactions on Audio, Speech, and Language Processing. 2015;23(1):162-173.
5. Townend O, Nielsen JB, Balslev D. SoundSense Learn: Listening intention and machine learning. Hearing Review. 2018;25(6):28-31.
6. Jensen NS, Hau O, Nielsen JBB, Nielsen TB, Legarth SV. Perceptual effects of adjusting hearing-aid gain by means of a machine-learning approach based on individual user preference. Trends in Hearing. 2019;23:1-23.
7. Balling LW, Townend O, Switalski W. Real-life hearing aid benefit with Widex EVOKE. Hearing Review. 2019;26(3):30-36.
8. Jensen NS, Balling LW, Nielsen JBB. Effects of personalizing hearing-aid parameter settings using a real-time machine-learning approach. In: Proceedings from the 23rd International Congress on Acoustics; September 9-13, 2019; Aachen, Germany.
9. Balling LW, Townend O. Using real-life data to improve real-life hearing. Audiology Practices. 2019;11(4):22-52.
10. Balling LW, Jensen NS, Caporali S, Cubick J, Switalski W. Challenges of instant-fit ear tips: What happens at the eardrum? Hearing Review. 2019;26(12):12-15.



