
The tinnitus population is massive and largely uninformed about treatment options—which includes significant benefit from properly fit hearing aids.
The size of the tinnitus population in the United States is nearly 30 million people—or about 10% of the entire population—and the incidence of tinnitus is as high as 26.7% for people ages 65-84 years. Data in this article also confirm that the provision of hearing aids offers substantial benefit to a significant number of people suffering from tinnitus. Evidence suggests that this information should be more widely disseminated in the audiological and medical communities.



Sergei Kochkin, PhD, is executive director of the Better Hearing Institute, Washington, DC. Richard Tyler, PhD, is professor in both the Department of Otolaryngology-Head & Neck Surgery and the Department of Communication Sciences and Disorders at the University of Iowa in Iowa City. He has authored numerous articles on the subject of tinnitus, and edited three books on the topic, the two most recent being Tinnitus Treatment: Clinical Protocols (Thieme) and The Consumer Handbook on Tinnitus (Auricle Ink Publishers). Jennifer Born is director of public affairs at the American Tinnitus Association (ATA), Portland, Ore, and also editor of ATA’s magazine, Tinnitus Today.
A number of estimates have been provided on the prevalence of tinnitus in the United States. Davis and El Refiae1 estimated that 10% to 15% of the US population experiences chronic or persistent tinnitus (eg, ringing in the ears or internal head noises). About half of the people with tinnitus are bothered by it, and it is reported that about 1% indicate that tinnitus substantially affects their lives. A recent self-report survey using the 1999-2004 National Health and Nutrition Examination Surveys (NHANES)2 database on more than 14,000 subjects estimated that 50 million US adults reported having any tinnitus and 16 million reported frequent tinnitus in the past year. Tinnitus was shown to increase with age, peaking at 14.3% of people ages 60 to 69 years. In addition, it was most prevalent among people with low-to-mid or high frequency hearing loss. Other authors indicate that chronic tinnitus affects 42 million Americans and is considered “clinically significant” in 10 million adults.3,4 It should be acknowledged that differences in the specific questions asked in these surveys likely account for much of the variability in numbers.
Tinnitus has been shown to have a direct impact on a person’s emotional well-being, hearing, and ability to sleep and to concentrate—in turn influencing basic life functions, such as socialization and relaxation.5,6 In severe cases, it can interfere with the individual’s ability to perform adequately on the job or contribute to psychological disorders, such as depression, suicide ideation, post-traumatic stress disorder, anxiety, and anger. The constancy of tinnitus and the perceived lack of control can provoke fear, which exacerbates the problem leading to an ever-increasing cycle of distress in the person suffering from tinnitus.7
Only a small number of people contact their physicians or hearing care professionals for help with their tinnitus. The reason perhaps lies in the widespread belief that tinnitus is incurable or untreatable. Yet, there are several methods for treating tinnitus that can alleviate the impact it has on the patient’s quality of life.6,8,9
In a large-scale study by the Better Hearing Institute (BHI), it was shown that 39% of people (more than 9 million adult Americans) indicated they had not sought help for their hearing loss specifically because they concurrently had tinnitus.10 It is likely their belief that tinnitus could not be treated influenced their decision not to seek treatment for either. Thus, those with both untreated tinnitus and untreated hearing loss would be expected to suffer an even greater diminished quality of life than individuals with just tinnitus or just hearing loss.
Tinnitus as a Professional Challenge
Since a substantial number of people with both tinnitus and hearing loss choose not to seek a solution for their hearing loss due to their tinnitus, we believe hearing care professionals must provide evidence that they can provide effective treatment for tinnitus. Most people with tinnitus also have a hearing loss. For those with hearing loss, hearing aids should obviously improve their hearing and communication. Hearing aids can help relieve tinnitus symptoms by improving communication, thereby reducing stress and making it easier to accept or cope with tinnitus.
Additionally, by amplifying background sound or producing background ambient noise, the loudness or prominence of tinnitus can be reduced. Hearing aids might be viewed as Gestalt therapy for the ears, since tinnitus (previously conspicuously in the foreground) is relegated appropriately to the background when environmental sounds are amplified. The very act of taking the focus off of tinnitus means relief for many people.
In a survey of 230 hearing care professionals, we specifically asked them to estimate the impact that using hearing aids had on their patients’ tinnitus.11 Their estimates were encouraging for those with tinnitus: 60% of their patients reported some relief of their tinnitus when using hearing aids, and 20% actually reported major relief of their tinnitus when using hearing aids.
Objective
The purpose of this paper is to determine the prevalence of tinnitus in a nationally representative sample of more than 46,000 households—the largest survey of its kind. We focused on quantifying tinnitus among people with hearing impairment, as well as those not reporting hearing impairment. This paper also explores, from the consumers’ perspective, the duration and intensity of their tinnitus and the impact it has on their quality of life. Furthermore, it examines treatment modalities designed to alleviate tinnitus and consumer perceptions of the efficacy of these treatments.
Survey Method
The Better Hearing Institute conducts a hearing health survey (MarkeTrak) of 80,000 households every 4 years using the National Family Opinion (NFO) panel. Typically, the survey focuses on people with hearing loss with detailed analysis of consumer experiences with hearing aids and supplemental analysis of hearing-impaired subjects not using hearing aids. In our 2008 survey, we specifically included questions about tinnitus.
In November and December 2008, a short screening survey was mailed to 80,000 members of the NFO panel. The panel consists of households that are balanced to the latest US census information with respect to market size, age of household, size of household, and income within each of the nine census regions, as well as by family versus non-family households, state (with the exception of Hawaii and Alaska), and the nation’s top-25 metropolitan statistical areas. In addition to questions previously asked and pertinent to other publications in the 2008 MarkeTrak series, we asked the panel head to indicate:
- Whether the household had one or more people “with a hearing difficulty in one or both ears without the use of a hearing aid”;
- Whether the household had one or more people who were the owner of a hearing aid;
- Whether the household had one or more people with tinnitus. For each question, the panel head checked off “none,” “self,” “spouse,” “other adult,” “child,” “dependent age 18 or over.”
This short screening survey was completed by 46,843 households. The response rate to the screening survey was 59%. In January 2009, an extensive 7-page legal size survey was sent to the total universe of hearing aid owners (3,789) in the panel database; 3,174 completed surveys were returned representing an 84% response rate.
In February 2009, an extensive 7-page legal survey was sent to a random sample of 5,500 people with hearing loss who had not yet adopted hearing aids (non-adopters). The response rate for the non-adopter survey was 79%.
Both hearing aid owners and non-adopters were given a $1 incentive to complete and return their surveys. Due to budgetary constraints, no detailed survey was sent to households where an individual was reported to have tinnitus but not hearing loss (because people with tinnitus typically have an accompanying hearing loss, it is likely this group had a mild hearing loss or a hearing loss outside of the range of normal audiometric testing, in additional to their tinnitus). Both hearing aid owners and hearing-impaired non-adopters were asked the following questions:
- Whether they were aware of tinnitus (defined as ringing or other sounds perceived in their ears or head).
- On a 0% to 100% scale, the duration of tinnitus in a day, loudness (0=faint, 100=very loud), and annoyance (0=not annoying at all, 100=extremely annoying or disabling).
- Areas of life negatively affected by tinnitus (7 areas).
- Treatments tried for tinnitus (9 treatments).
- Efficacy of tinnitus treatments on 0-100% scale (0=not effective at all, 100=completely effective).
For hearing aid owners, we asked them:
- To rate the impact of hearing aids on their tinnitus on a 5-point scale: 1=made tinnitus worse, 2=no effect, 3=mild reduction in loudness or awareness, 4=moderate reduction in loudness or awareness, 5) significant reduction in loudness or awareness.
- If hearing aid owners indicated a mild, moderate, or significant reduction to their tinnitus using hearing aids, we asked them to tell us how often they experienced this reduction: 1=occasionally, 2=frequently, 3=most of the time, 4=all of the time while wearing hearing aid, 5=all of the time even when not wearing their hearing aid.
The data presented in this article refer only to households as defined by the US Bureau of Census; that is, people living in a single-family home, duplex, apartment, condominium, mobile home, etc. People living in institutions have not been surveyed; these would include residents of nursing homes, retirement homes, mental hospitals, prisons, and the military.
Hearing loss demography and segmentation into deciles. Both aided and unaided subjects were asked to complete the following subjective measures of hearing loss. They were then segmented into 1 of 10 groups (called deciles) based on their responses to five measures of hearing loss:
- Number of ears impaired (1 or 2).
- Score on the Gallaudet Scale.12 An 8-point scale in which the respondent indicated whether they can understand speech under the following conditions: “whisper across a quiet room,” “normal voices across a quiet room,” “shouts across a quiet room,” “loud speech spoken into their better ear,” “not able to understand loud speech in their better ear”; in addition, “tell noises from each other,” “hear loud noises at all,” “hear any sound or any noise.” An individual’s score ranged from 1 to 8. Typically, they are classified into 1 of 5 groups (1=hear whisper, 2=hear normal voice, 3=hear shouts, 4=hear speech in better ear, 5=can’t hear speech). What makes the Gallaudet Scale of particular value is it has been validated against clinical information (dBHL loss in better ear). The Gallaudet Scale has historically been used by the Centers for Disease Control and Prevention in their quantification of the hearing-impaired population.
- Subjective hearing loss score. The respondent subjectively evaluated their hearing loss as “mild,” “moderate,” “severe,” or “profound.” This measure is given a score of 1 (mild) to 4 (profound).
- Difficulty hearing in noise. This 5-point scale runs from “extremely difficult” hearing in noise to “not at all difficult” and is based on the work of Plomp.13
- BHI Quick Hearing Check. This 15-item, 5-point Likert scaled hearing loss inventory is based on the revised American Academy of Otolaryngology-Head & Neck Surgery (AAO-HNS) 5-minute hearing test14,15 and has been shown to be correlated with both subjective and objective measures of hearing loss.
A factor analysis of the above subjective measures was performed, revealing a single subjective measure of hearing loss. Factor analysis is a method for extracting common variance among multiple variables. A composite hearing loss score was determined by computing factor scores for hearing aid owners and non-adopters. Based on their score, they were placed into 1 of 10 hearing loss groups where Decile 1 represented the mildest hearing loss (ie, the lower 10% of people with hearing loss) and Decile 10 represented the most serious hearing loss (ie, the top 10% of people with hearing loss). Finally, the data was weighted to reflect hearing aid owners and non-adopters in the general population. With respect to the BHI Quick Hearing Check, subjects were placed into quintiles for this study based on extensive US norms reported elsewhere.15
Best practices. In an extensive article16 published in the April 2010 edition of Hearing Review, 17 hearing care best practices were correlated with hearing aid user success, and an overall index (z score with mean=5, std=2) of best practices in fitting hearing aids was derived. In the present study, we will reveal the relationship between best practices in fitting hearing aids and the efficacy of tinnitus mitigation with hearing aids. A high best-practice rating indicates the services included such things as:
- Hearing tests conducted in a sound booth;
- Use of probe microphones in verifying the hearing aid fitting;
- Validation of the hearing aid fit with objective and subjective outcome measures;
- Loudness discomfort measurement;
- Counseling;
- Skillful use of software;
- Consumer feedback in achieving optimum sound quality of the hearing aid and hearing aids that fit the consumer comfortably.
The reader is referred to the earlier paper16 for a detailed description of best practices measurement methodology.
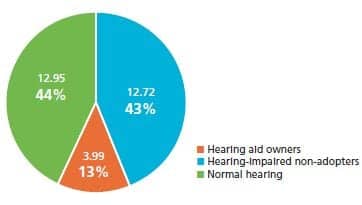
Figure 1. Tinnitus population (millions, 2008)
RESULTS
Prevalence of Tinnitus
Table 1 details the demography of the population of people reporting tinnitus. In the first section, and graphically portrayed in Figure 1, the tinnitus population is documented based on their reported usage of hearing aids and awareness of hearing loss, tinnitus, or both. The 2008 tinnitus population is estimated at 29.7 million people. Nearly 4 million were current hearing aid owners; this represents 47% of the 8.4 million hearing aid owners in the United States.17 Slightly more than 2 of 5 (42.9%) people with tinnitus are hearing-impaired subjects who do not use hearing aids (non-adopters, representing nearly half of the 25.8 million non-adopters).17
Surprisingly, nearly 44% of subjects (12.95 million) with tinnitus report no hearing loss. It is generally agreed that most people with tinnitus have at least a mild hearing loss.18 To these subjects, tinnitus might have been more noticeable than actual hearing loss. Their hearing loss might have been mild and not had a dramatic influence on listening, or they chose not to acknowledge it. Thus, the known hearing loss population of 34.25 million17 may in fact be closer to 47 million.
Referring back to Table 1, the percent distribution of people with tinnitus by demography is shown along with the size of the tinnitus population (in thousands), and the total percent distribution within the US population. The final column is the ratio of the tinnitus distribution divided by the US population distribution (from the Bureau of Census).19 Figures higher than 100 mean that tinnitus in the demographic segment is higher than the population segment.
The average age of people with tinnitus is 57. The tinnitus population size peaks at 7.2 million people in the ages 55-64 year bracket and the tinnitus ratio (actual/US population) is nearly 3 times the expected level for the age bracket 65-84.
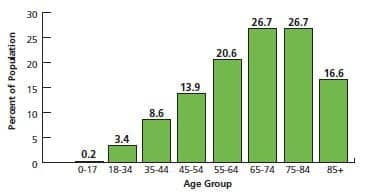
Figure 2. Incidence of tinnitus by age group. Incidence derived by comparing age population from NFO panel with U.S. Bureau of Census population in 2008
Figure 2 plots the incidence of tinnitus by age group. Tinnitus is shown to be highly related to age of the subject with a low of 0.2% for people under age 17 years and a high of 26.7% for people between ages 65 and 84 years. The incidence for subjects 85+ years is shown to decrease to 16.6%, probably due to the factors that involve the NFO panel. It should be remembered that the NFO panel does not sample people in nursing homes, and that the head-of-household filling out the survey may be aware of hearing loss but not necessarily aware of tinnitus in elderly people living in their household.
People with tinnitus are more likely to have an education below high school; to be retired, disabled, or on medical leave; to have lower household incomes; to live in smaller rural communities; and to be single. Referring to Table 2, all hearing loss characteristics, except number of ears impaired, are statistically correlated with the presence of tinnitus. While people with more severe hearing loss are more likely to have tinnitus, the data shows that tinnitus is a condition held also by people with milder hearing losses. For example, nearly 1 in 4 people with hearing loss report their hearing loss as “mild,” 51% can hear a whisper or normal speech without visual cues, 31% are in the two lower quintiles (bottom 40%) of hearing loss as measured by the BHI Quick Hearing Check, and 17% are in the two lower deciles of hearing loss (bottom 20%) when you consider all subjective hearing loss measures in this study.
Severity of TInnitus
We measured tinnitus severity in three ways: duration of day tinnitus is present, loudness of tinnitus on a 100% scale (faint to loud), and annoyance of tinnitus on a 100% scale (not annoying to disabling). The results from 3,374 respondents are shown in Table 3. On average, people with tinnitus are aware of their tinnitus about half the time. Less than 4% would describe their tinnitus as intermittent (0% response), while about one-third experience their tinnitus less than 20% of the time in a typical day. Nearly 4 in 10 (39.1%) people experience their tinnitus 80% or more of the day.
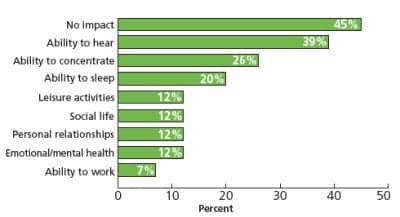
Figure 3. Impact of tinnitus on quality of life (n=3,431)
The average person rated their tinnitus at 41% on our loudness scale. Approximately 13% of subjects describe their tinnitus as faint (0% to 19% rating), while 21.6% described their tinnitus as loud (70% to 100%).
The average person rated their tinnitus at 39% on our annoyance scale. Approximately 1 in 10 describe their tinnitus as not annoying at all, while 22.2% describe their tinnitus as disabling or nearly disabling.
In Figure 3, respondents shared with us the impact their tinnitus has on their life. Nearly half (45%) indicate their hearing loss has no impact on their life. About 2 in 5 (39%) report that tinnitus affects their ability to hear, 1 in 4 (26%) their ability to concentrate, and 1 in 5 their ability to sleep. A small minority of subjects (12%) indicate that tinnitus affects their leisure activities, social life, personal relationships, and emotional or mental health. A total of 7% indicate that tinnitus affects their ability to work.
InTable 4 we have segmented the quality of life impact of tinnitus based on the severity of tinnitus. An index of severity of tinnitus was derived through factor analysis of the duration of tinnitus, annoyance, and loudness of tinnitus. Factor scores were standardized to a mean of 5 and standard deviation of 2. As an example, subjects with mild tinnitus (score of 2) indicate that their tinnitus affects their ability to hear 9% of the time, while subjects with the most severe tinnitus (score of 9) indicate that their tinnitus affects their ability to hear 75% of the time.
Efficacy of Treatment Methods
Subjects with tinnitus were presented with a list of nine methods of treating tinnitus and asked if they tried those techniques to treat their tinnitus (Table 5). They were then asked to rate the efficacy of those treatments in mitigating tinnitus on a 0% to 100% scale. The range of methods tried varied from a low of 1% (wearing sound generators) to use of herbs and dietary supplements (6.8%). Only 6.1% (n=212) indicated they had used hearing aids to treat their tinnitus. With respect to hearing aids, we also directly queried the impact hearing aids had on their tinnitus, yielding a much larger sample of 1,314 responses.
The data in Table 5 are sorted by mean efficacy; however, since all treatment methods are skewed toward “no effect,” a more realistic indication of value is the median. The highest rating was achieved by hearing aids (34%) and music (30%) followed by relaxation techniques (10%). Focusing on substantial-to-complete amelioration of tinnitus (ie, >80% of symptoms), hearing aids were rated the highest (27%), followed by music (20%). Approximately 1 in 10 experienced substantial relief of their tinnitus through medication from their physician, relaxation techniques, counseling, or a non-wearable sound generator.
The results of our direct query on hearing aid efficacy are shown in Figure 4. More than half (52.4%) indicated that hearing aids had no effect, while only 4.2% indicated that hearing aids made their tinnitus worse. Nearly 3 out of 10 (27.8%) indicated they received moderate-to-substantial reduction in their tinnitus through the use of hearing aids, while nearly 16% received a mild reduction in their tinnitus.
Subjects reporting mild-to-substantial mitigation of tinnitus reported on how often hearing aids impacted their tinnitus (Figure 5). Nearly 2 out of 3 subjects reported hearing aids relieved their tinnitus most of the time to all of the time, while 3 out of 10 (29%) reported that hearing aids alleviated their tinnitus all of the time.
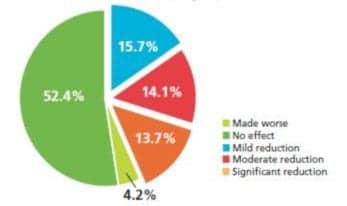
Figure 4. Effectiveness of hearing aids in mitigating effects of tinnitus (n=1,314)
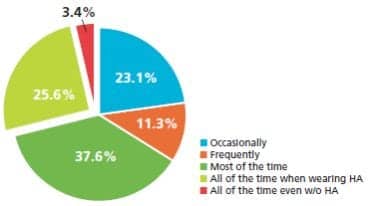
Figure 5. How often hearing aids are effective in mitigating effects of tinnitus (n=553)
Subjects Experiencing Tinnitus Mitigation With Hearing Aids
It is of considerable interest to understand who benefits from tinnitus relief through the use of hearing aids. In ,Table 6 we have documented levels of tinnitus relief. Age, level of hearing loss, and severity of hearing loss are not related to how often the respondent experiences relief from tinnitus while wearing hearing aids. However, degree of hearing loss and severity of tinnitus are significantly related to level of tinnitus reduction via hearing aid use. In general, people with milder degrees of tinnitus are more likely to experience mitigation of their tinnitus with hearing aids.
In an earlier publication,16 it was demonstrated that providing comprehensive audiological services (“best practices”) when fitting hearing aids resulted in a significant benefit on real-world success with hearing aids. In Table 7, we document the level of importance of specific hearing aid fitting practices relative to the effectiveness of hearing aids in achieving tinnitus mitigation.
We acknowledge that there are other “best practice” procedures not measured in this study specifically applicable to the treatment of tinnitus.20 However, the evidence presented in Table 7 and Figure 6 leads one to conclude that, if comprehensive audiological services are used to fit hearing aids, there is a stronger probability that the subject with tinnitus will derive benefit from their hearing aids to treat their tinnitus.
Factors demonstrating both statistical and practical significance for a comprehensive/best practice (meaningful trend from made worse/no effect to significant tinnitus reduction) are:
- Use of real-ear measurement in fitting the hearing aid;
- Objective benefit measurement;
- Customer satisfaction measurement;
- Loudness discomfort measurement;
- Hearing aid fit and comfort;
- Achieved sound quality (composite measure of seven ratings by the consumer); and
- Attributes of the hearing health professional (composite measure of seven ratings by the consumer).
Considering the entire hearing aid fitting weighted protocol (composite measure of 17 factors, mean=5, std=2), subjects reporting their hearing aids made their tinnitus worse received a “best practice” rating of 3.4; in comparison, subjects reporting significant improvement in their tinnitus received a “best practice” rating of 5.7.
Finally, we segmented the sample into five quintiles (20% groupings) based on the overall best practice score. As shown in Figure 6, subjects receiving a more comprehensive hearing aid fitting protocol (Quintile 5) are nearly twice as likely to experience tinnitus relief from their hearing aids than if they received a minimalist hearing aid fitting protocol (Quintile 1).
Discussion
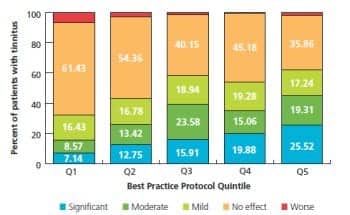
Figure 6. Tinnitus mitigation with hearing aids segmented by best practice hearing aid fitting score in quintiles where Q1=bottom 20% of practices and Q5=top 20% of practices (n=732)
Tinnitus prevalence. Following the model of Tinnitus Activities Treatment,20 tinnitus influenced hearing in 39%, concentration in 26%, sleep in 20%, and emotions in 12% of subjects reporting tinnitus. Tinnitus also influences secondary factors, though to a lesser extent.21 In this study, tinnitus negatively impacted leisure activities in 12%, socialization in 12%, personal relationships in 12%, and work in 7% of people with tinnitus. The fact that tinnitus can have a major impact on work performance is of substantial importance to society at large and not always widely appreciated.
We estimate that 10%—or 29.7 million people—of the United States population have tinnitus, and for the majority this was persistent tinnitus. We define tinnitus as the sensation of an unwanted sound in one or both ears in the absence of any outside auditory stimulus. The population sampled was nearly 47,000 representative households but did not include people living in institutions. We should note that our tinnitus estimates are based on responses from the head of the households; however, for subjects with reported hearing loss (aided or unaided), the information about their tinnitus was received directly from the individual with tinnitus in a detailed follow-up survey.
This estimated tinnitus prevalence of 10% is in excellent agreement with many previous epidemiological studies (as reviewed in the introduction). It highlights the extremely common occurrence of tinnitus throughout the population. Demographically, an increase in incidence of tinnitus was found in people with a lower education; who were retired, disabled, or on health-related leave from work; with lower household incomes; living in smaller rural communities; and single in marital status.
The main limitation of this study is it did not include people living in institutions such as nursing homes and military facilities. Because tinnitus is correlated with age and hearing loss, the incidence of tinnitus is conceivably higher when we consider the nursing home population. In fact, among elderly subjects greater than age 80 living with younger family members, the data in Figure 2 would indicate that family members may not be aware of tinnitus in their elderly household members. In addition, it is widely known that tinnitus impacts many veterans and military personnel. At the end of 2010, tinnitus was the leading service-connected disability for veterans from all periods of service.22
Tinnitus treatment and under-utilization of hearing aids. It is surprising that so few patients had tried treating their tinnitus at all, and a large number of people did not view hearing aids as a treatment method. This might reflect the general adage that “there is nothing you can do about it!” Hearing care professionals and their allied professional organizations need to promote that there are many successful counseling and sound therapy options, including hearing aids, that can help tinnitus patients.
The most-common treatment patients had tried was herbs and dietary supplements (6.8%) followed by hearing aids (6.1%). Remarkably, only 1% had tried sound generators to treat their tinnitus. This is most unfortunate, as our clinical experience is that many patients benefit from these devices. There is data questioning the efficacy of sound therapy, but these studies typically set the maskers to approximate the level of the tinnitus (the mixing point) or used total masking; our experience is that these levels are too high for most patients.23 There are data supporting the benefit of sound therapy.24
It is also surprising that only about 6.1% report having used hearing aids to treat their tinnitus. In our larger sample of hearing aid users (n=1,314)—when we directly queried the use of hearing aids—almost half indicated that their hearing aids provided mild-to-significant tinnitus relief! And, for those experiencing tinnitus mitigation, the majority reported relief most of the time to all of the time.
This is an important benefit that should be more widely acknowledged. Most encouraging is the fact that only about 4% of subjects indicated that their hearing aids made their tinnitus worse. Careful hearing aid fitting is required in tinnitus patients—perhaps reducing the maximum output of the hearing aids.8 Hearing-impaired people should be made aware that the use of hearing aids could very well provide additional benefits to their tinnitus, over and above the important benefit to communication.
About one-third of the small sample of subjects using music to treat their tinnitus (3.4%) reported substantial benefit. Of course, music is often helpful for tinnitus sufferers getting to sleep, and it has been widely appreciated in the literature. The use of music, including other variants and custom forms of sound, can be a very helpful way to alleviate tinnitus. About 10% of our sample stated they specifically used relaxation techniques to help relieve their tinnitus.
There is little evidence in this study that medication from physicians, relaxation techniques, counseling, or herbal supplements helped except in a very small minority of subjects with tinnitus.
Noise exposure is the leading cause of tinnitus, and in individuals who develop tinnitus this way, there is also usually an accompanying hearing loss. The incidence of tinnitus is expected to grow due to our noisy society, the aging of America, and the return of military veterans. There have been several recent studies that have found higher incidences of tinnitus in young adults, teenagers, and children. In the first large, national, population-based study, it was estimated that 12.5% of children ages 6 to 19 years have noise-induced threshold shifts, accounting for nearly 13 million children and young adults in the United States.25 However, the authors believe the threshold shifts were very small in this study, and the causative link between noise and slight hearing loss was not established.
Summary of Findings
- The size of the tinnitus population in the United States is nearly 30 million people—or about 10%.
- 13 million people report they have tinnitus but not hearing loss. However, it is widely acknowledged that people with tinnitus almost always have hearing loss. Therefore, it is likely that the hearing loss population is conceivably higher than previously reported.
- The incidence of tinnitus is as high as 26.7% for people ages 65-84 years.
- The prevalence of tinnitus is correlated with degree of hearing loss; however, it is clear that all levels of hearing loss (mild to severe) can experience tinnitus.
- Nearly 4 in 10 people experience their tinnitus >80% of the time during a typical day; slightly more than 1 in 4 people describe their tinnitus as loud; and about 1 in 5 describe their tinnitus as disabling or nearly disabling.
- Subjects with tinnitus report their tinnitus primarily impacts their ability to hear (39%), concentrate (26%), and sleep (20%).
- Of the nine tinnitus treatment methods assessed, none were tried by more than 7% of the subjects. Treatment methods rated with substantial tinnitus amelioration were hearing aids (34%) and music (30%).
- In a direct query of hearing aid efficacy, 27.8% of hearing aid users reported receiving moderate-to-substantial reduction in their tinnitus when using their hearing aids. About 2 out of 3 people experienced tinnitus relief most of the time to all of the time, while 3 out of 10 (29%) reported that the use of hearing aids alleviated their tinnitus all of the time.
- Subjects who had their hearing aids fit by professionals using comprehensive hearing aid fitting protocols are nearly twice as likely to experience tinnitus relief than respondents fit by hearing care professionals using minimalist hearing aid fitting protocols.
- Almost one-quarter of those with tinnitus describe their tinnitus as disabling or nearly disabling. There is currently no cure. This study confirms that the provision of hearing aids offers substantial benefit to a significant number of people suffering from tinnitus. This fact should be more widely acknowledged in both the audiological and medical communities.
Table 1. Tinnitus Population Demography (n=8,608). Comparison is distribution of tinnitus population versus total US population.
* Total US population distribution from Bureau of Census for age and gender; the remainder from the entire NFO panel.
Table 2. Hearing loss characteristics of people reporting they have tinnitus versus those who do not have tinnitus.
Data includes only those reporting they have a hearing loss.
Table 3. Severity of Tinnitus, 0-100% scale (n=3,374).
Table 4. Impact (%) of tinnitus on quality of life segmented by severity of tinnitus (n=3,187).
Severity of tinnitus is the factor score of duration, annoyance, and loudness of tinnitus. The composite measure is standardized to a mean=5, std=2.
*Note correlation with factor score = Time of day (.74), annoyance (.87), loudness (.91)
Table 5. Treatments tried for tinnitus and efficacy on 0-100% scales (3,473).
Table 6. Profile of hearing aid users and the mitigating impact on tinnitus due to hearing aids.
Table 7. The impact of best practices on tinnitus mitigation with hearing aids (hearing aids < 4 years of age).
Acknowledgements
This study was made possible by a special grant from Knowles Electronics Inc, Itasca, Ill.
Correspondence can be addressed to Sergei Kochkin, PhD, at.
References
- Davis A, El Refaie A. Epidemiology of tinnitus. In: Tyler RS, ed. Tinnitus Handbook. San Diego: Singular Publishing Group; 2000:1-24.
- Shargorodsky J, Curhan GC, Farwell WR. Prevalence and characteristics of tinnitus among US adults. Am J Med. 2010;123(8):711-718.
- Henry JA, Dennis KC, Schechter MA. General review of tinnitus: prevalence, mechanisms, effects, and management. J Speech Lang Hear Res. 2005;48:1204-1235.
- Hoffman HJ, Reed GW. Epidemiology of tinnitus. In: Snow JB, ed. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004.
- Erlandsson S. Psychological profiles of tinnitus in patients. In Tyler RS, ed. Tinnitus Handbook. San Diego: Singular Publishing Group; 2000:25-58.
- Tyler R. Neurophysiological models, psychological models, and treatments for tinnitus. In: Tyler R, ed. Tinnitus Treatment. New York: Thieme; 2006.
- Noble W, Tyler R. Physiology and phenomenology of tinnitus: implications for treatment. Int J Audiol. 2007;46(10):569-575.
- Searchfield GD. Sound therapy options. In: Tyler R, ed. The Consumer Handbook on Tinnitus./ Sedona, Ariz: Auricle Ink Publishers; 2008.
- Jastreboff PJ, Hazell JWP. Tinnitus Retraining Therapy: Implementing the Neurophysiological Model. Cambridge, UK: Cambridge University Press; 2004.
- Kochkin S. MarkeTrak VII: Obstacles to adult non-user adoption of hearing aids. Hear Jour. 2007;60(4):27-43.
- Kochkin S, Tyler R. Tinnitus treatment and the effectiveness of hearing aids: hearing care professional perceptions. Hearing Review. 2008;15(13):14-18.
- Schein JD, Gentile A, Haase KW. Development and evaluation of an expanded hearing loss scale questionnaire. National Center for Health Statistics. Vital Health Stat 2. 1970 Apr;(37):1-42.
- Plomp R. Auditory handicap of hearing impairment and the limited benefit of hearing aids. J Acoust Soc Am. 1978;63:533-549.
- Koike J, Hurst MK, Wetmore SJ. Correlation between the American Academy of Otolaryngology-Head & Neck Surgery (AAOHNS) five minute hearing test and standard audiological data. Otolaryngol-Head Neck Surg. 1985;111(5):625-632.
- Kochkin S, Bentler R. The validity and reliability of the BHI Quick Hearing Check. Hearing Review. 2010;17(12):12-28.
- Kochkin S, Beck D, Christensen L, et al. MarkeTrak VIII: The impact of the hearing healthcare professional on hearing aid user success. Hearing Review. 2010;17(4):12-34. Accessed May 27, 2011.
- Kochkin S. MarkeTrak VIII: 25 year trends in the hearing health market. Hearing Review. 2009;16(11):12-31.
- Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord 1990;55(3):439-453.
- US Bureau of Census age and sex distribution, 2008. Available at: www.census.gov/population/www/socdemo/age/age_sex_2008.html. Accessed September 28, 2011.
- Tyler RS, ed. Tinnitus Treatment: Clinical Protocols. New York: Thieme; 2006.
- Tyler RS, Noble W, Coelho C, Haskell G, Bardia A. Tinnitus and hyperacusis. In: Katz J, Burkard R, Medwetsky L, Hood L, eds. Handbook of Clinical Audiology. 6th ed. Baltimore: Lippincott Williams & Wilkins; 2009.
- Department of Veterans Affairs, Veterans Benefits Administration. Annual Benefits Report, FY 2010:5. Available at: www.vba.va.gov/REPORTS/abr/index.asp. Accessed September 28, 2011.
- Tyler RS, Bentler RA. Tinnitus maskers and hearing aids for tinnitus. Seminars in Hearing. 1987;8(1):49 61.
- Davis PB, Wilde RA, Steed LG, et al. Treatment of tinnitus with a customized acoustic neural stimulus: a controlled clinical study. Ear Nose Throat J 2008;87:330-339.
- Niskar AS, Kieszak SM, Holmes AE, Esteban E, Rubin C, Brody DJ. Estimated prevalence of noise-induced hearing threshold shifts among children 6 to 19 years of age: The Third National Health and Nutrition Examination Survey, 1988–1994, United States. Pediatrics. 2001;108:40-43.
Citation for this article:
Kochkin S., Tyler R., Born J. MarkeTrak VIII: The Prevalence of Tinnitus in the United States and the Self-reported Efficacy of Various Treatments Hearing Review. 2011;18(12):10-27.



