
Tech Topic | March 2015 Hearing Review
A look at the long-term effectiveness of an integrated tinnitus management approach (WZT) and the pattern of amplification and sound therapy use among primary tinnitus patients once successful remediation of symptoms is achieved.
A recent publication described the effectiveness of Widex Zen Therapy (WZT).1 In this paper, we report the results of a study designed to determine the long-term outcome of this tinnitus management approach and to examine the usage patterns of amplification and/or sound therapy once the patient has achieved a satisfactory resolution or believes habituation has occurred.

Robert W. Sweetow, PhD
Habituation is classically defined as the process of adapting to a stimulus through repeated exposure. When tinnitus habituation occurs, either the perception of the tinnitus, or the reaction to the tinnitus, is greatly, if not fully, diminished.2 In this article, habituation will be regarded as substantial and meaningful lessening of the negative reaction to the tinnitus as defined by clinically significant reductions in subjective distress scores.

Melodi Fehl, MA
Tinnitus is one of the most common and distressing otologic symptoms. The reaction to it varies from a minor annoyance to one that can significantly and negatively impact one’s quality of life. The condition typically involves multiple neuro-plastic changes to sites producing auditory, attentional, and emotional processes of the brain.

Patricia M. Ramos, AuD
The attentional processes involve perceptual filters that determine which sensory perceptions are brought to our conscious attention. In clinically significant tinnitus, these filters determine that attention should be applied to the specific patterns of neural activity associated with the tinnitus.3,4 The engagement of the autonomic system and amygdala leads to further increases in the sensitivity of the auditory system and reinforcement of the attentional filters, creating further increase in tinnitus loudness and awareness, which in turn increases the level of stress. The mechanisms of emotional disturbance associated with tinnitus define the “reaction” to hearing the tinnitus sound, as opposed to the “perception” of the sound.
The vast majority of tinnitus patients present at least some degree of hearing loss, fueling the theory that the central auditory nervous system responds to the hearing deficit by increasing its gain, further adding to the perception of tinnitus. Audiologists have long recognized the value of using hearing aids in the management of tinnitus5; however, the percentage of tinnitus patients who require amplification is unclear due to the wide range (20-90%) cited in various reports.6-9
The use of music has been shown to reduce stress hormones.10 Physiological and behavioral reactions to tinnitus can be mitigated through the use of music. More generally, sounds perceived as relaxing can reduce stress. Thus, sound therapy targeting the relaxation response can be an important component of a tinnitus management program.5
Hearing aids with either noise generators or some kind of music have become popular in tinnitus management. A limitation of the use of popular music, however, is the chance that these stimuli can attract excessive attention to both the music and the tinnitus. Auditory fractal tones utilize harmonic but unpredictable musical relationships, and are generated by a recursive process where the algorithm is applied multiple times to process its previous output. The chime-like tones are pleasant, but are not associated with music that the listener may hold in memory; thus the presence of the fractal tones produces a greater likelihood of passive listening.11 The use of fractal tones and amplification have been reported in several papers,12-15 all reporting favorable results with regard to reducing the tinnitus distress or enhancing relaxation.
Consequently, there is a growing consensus that a multifaceted individualized approach to tinnitus management is more likely to result in the best outcomes. Most tinnitus strategies employed over the past two decades consist of a combination of directive (instructional) counseling and acoustic stimulation (either noise, amplification, or a combination of the two). Widex Zen Therapy extends these approaches by additionally incorporating cognitive behavioral interventions in the form of adjustment-based counseling designed to identify the unwanted thoughts and behaviors hindering natural habituation, challenge their validity, and replace them with alternative and logical thoughts and behaviors.
In addition, WZT incorporates the use of fractal (commercially termed Zen) tones and broadband amplification characterized by an extremely low compression kneepoint, relaxation exercises, and sleep management. There is also an option to include broadband noise in addition to, or in lieu of, the Zen tones. The approach is individualized, in that the necessary components of WZT are determined after a comprehensive evaluation of the tinnitus and the patient’s reaction. Typically, the more severe and negative tinnitus reaction, the more components are added. The overall aim of Widex Zen Therapy is to ensure that the tinnitus does not negatively impact the patient’s quality of life, as opposed to reducing the loudness level or production of the tinnitus. Detailed descriptions of WZT are available.16,17
The effectiveness of WZT in several studies has been reported,1,18-19 but none of these investigations have indicated the effectiveness or usage characteristics beyond a 6-month period. Thus, the objectives of this investigation were to:
1) Determine the long-term outcome of the WZT tinnitus management approach, and
2) Examine the pattern of use of amplification and/or sound therapy following a satisfactory resolution or belief that habituation has occurred.
Research Methodology

Figure 1. Average thresholds and 1 standard deviation for the 19 subjects are shown.
Participants. A total of 20 subjects were initially enrolled in this cohort study conducted at the ENT Associates of South Florida in Boca Raton, Fla. All but one (19 subjects, 11 females and 8 males with a mean age of 65, ranging from 49 to 86) completed the study. Seventeen of the subjects initially presented to the clinic with a primary complaint of tinnitus, rather than hearing difficulty. All but 7 subjects had experienced tinnitus for more than 1 year, and all but 4 reported tinnitus in both ears.
All but one of the subjects were first-time hearing aid users (N=18). The hearing loss varied from mild to moderately severe, and the average hearing thresholds of the subjects are shown in Figure 1.
All participants were given a comprehensive audiologic and tinnitus evaluation including the Tinnitus Handicap Inventory (THI),20 Tinnitus Functional Index (TFI),21 and Widex Tinnitus Intake questionnaire.17 Participants were required to have cognitive, comprehension, and manual dexterity abilities sufficient for treatment, and all subjects paid for the tinnitus treatment for up to 12 months post hearing aid fitting. Participants received medical clearance and signed consent forms.
All subjects had significant tinnitus distress (THI >18) when they initiated the clinical study with mean scores of 60 (range: 28-88) on the TFI, and 55 (range: 20-82) on the THI. The mean tinnitus loudness was 6 (±1.7) on a 10-point Likert scale, and the tinnitus pitch was 7 (±2.7), indicating that the tinnitus pitch was mostly at high frequencies at the pre-treatment session. Thirteen subjects had received previous tinnitus treatments.
Procedures. Clinicians participating in this investigation had considerable experience in tinnitus patient management and were familiar with the fitting of Widex hearing aids and Zen programming. The Widex Intake Questionnaire, TFI, THI, and the clinician’s observation of the subjects were used to determine which WZT components were employed. All subjects were given instructional counseling, relaxation exercises including progressive muscle relaxation (PMR), deep breathing and guided imagery, and sleep suggestions. Additional counseling in the form of cognitive behavioral intervention was applied when the clinicians believed appropriate.
Additionally, all subjects were fit with Widex Dream or Clear hearing aids containing fractal (Zen) tones. The specific models chosen ranged from models 110 to 440, and were selected based on the joint decision of the patient and clinician taking in audiologic as well as economic considerations. The hearing aids had wide dynamic range compression (WDRC), compression thresholds as low as 0 dB HL, adaptive multichannel directional microphone, noise reduction, active feedback cancellation, data logging, and inter-ear capabilities.
The hearing aids were initially programmed in accordance with the hearing loss, and included the Zen + program with multiple options:
- A) Aqua + microphone on;
- B) Aqua + microphone on + noise; and
- C) Zen noise + microphone on.
Zen + A (aqua) was recommended for quiet situations in order to avoid silence. Zen + B (noise) or Zen noise (C) were only recommended if the clients experienced periods where the tinnitus was very bothersome.
Even though the initial fitting met most subjects’ needs, some required individual modifications in their Zen + programming. Although turning off the microphone in the Zen+ programs was an option, only two subjects chose to do so.
Subjects were instructed to use the devices during their waking hours when hearing and communication were essential. They were further taught that the Zen fractal tones should be audible, but relatively soft and that the tones should not interfere with conversational speech. Thus, the volume was to be set so that the annoyance level of the tinnitus would just begin to decrease. A more detailed explanation of the Zen programming is available.17 Subjects were advised to not adjust the Zen volume unless deemed necessary by environmental conditions.
Outcome measures. The TFI and THI were administered at baseline, as well as at 2, 4, 6, 9, and 12 months post-treatment. Hearing aid datalog records were accessed at these time intervals to ascertain hearing aid use both during the therapeutic effort to induce habituation and after. The number of sessions necessary to accomplish a successful outcome varied and was defined by a clinically significant reduction in THI and TFI scores, or achievement of a non-significant score (< 20 for the TFI or less than 18 for the THI) for two consecutive visits, as well as a subjective report that tinnitus awareness, or tinnitus disturbance, or quality of life was no longer an issue negatively impacted by the tinnitus. Subjects who showed clinically and significantly improvements didn’t require all the planned sessions; however, the THI, TFI, and datalogging measures were still collected as planned.
Results
Because there were strong positive correlations (r = >.77; p = 0.001) found between the TFI and THI results for all visits, and in the interest of brevity, only the TFI data will be presented below. The TFI was chosen because of its extremely strong psychometric evidence and multiple domain clinical relevance.

Figure 2. Mean Tinnitus Functional Index scores at baseline, 2, 4, 6, 9, and 12 months. Bars represent standard error.
The mean TFI at baseline was 60 (range: 28-88) and the mean score after 12 months of WZT was 12 (range: 0-54). The mean improvement was 48 points (Figure 2). A repeated measures ANOVA showed that visit was a significant factor (p<0.001). Post hoc analysis using a paired-sample t-test showed the mean TFI at 2 months was significantly lower than that recorded at the baseline (p<0.001). There was also a significant reduction at the 6-month visit compared to the 4-month visit (p<0.05). Though there were continuous improvement in TFI scores observed over the 12-month course of this investigation, the reductions in scores between the 2- and 4-month visits and between the 6- and 12-month visits were not statistically significant (p>0.05). Thus, the largest mean change (32) in TFI scores was obtained after 2 months of WZT. In addition, it should be noted that the final mean TFI score was 11.76, a tinnitus distress score considered clinically insignificant.

Figure 3. Individual subject Tinnitus Functional Index (TFI) baseline and 12 month post Widex Zen Therapy scores for the 19 subjects. The solid line represents equivalent scores. The dashed line represents the 13-point benefit score considered clinically significant.
Figure 3 depicts the relationship between TFI baseline and 12-month post WZT for individual subjects. The solid diagonal line reflects equivalent pre and post scores. Any symbol falling below this diagonal line suggests some degree of reduction in tinnitus distress. A reduction of 13 points is considered clinically significant on the TFI.21 The dashed line represents the 13-point benefit score considered clinically significant. Symbols falling below the diagonal dashed line reflect clinically significant relief from tinnitus. Thus, all 19 subjects had clinically significant improvements in their TFI scores. In addition, 15 of the 19 subjects’ final TFI were below the 20-point score considered clinically significant.
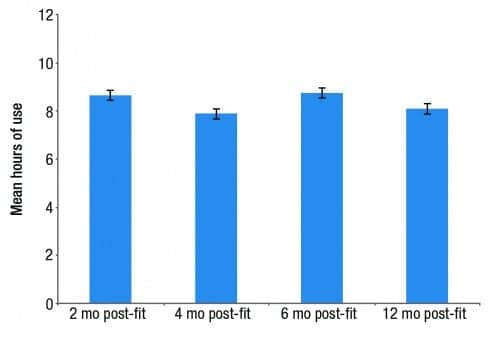
Figure 4. Mean hours of hearing aid use at 2, 4, 6, and 12 months. Bars represent standard error.
Hearing Aid Use. Hearing aid datalog information was collected during visits at 2, 4, 6, 9, and 12 months. The mean use of hearing aids, including amplification and Zen programs, was 8 hours during the 12-month course of this investigation. As depicted in Figure 4, there was little or no change in the use of hearing aids for the follow-up visits after the first 2 months, as confirmed by the non-significant statistical differences found on a repeated-measures ANOVA (p>0.05).
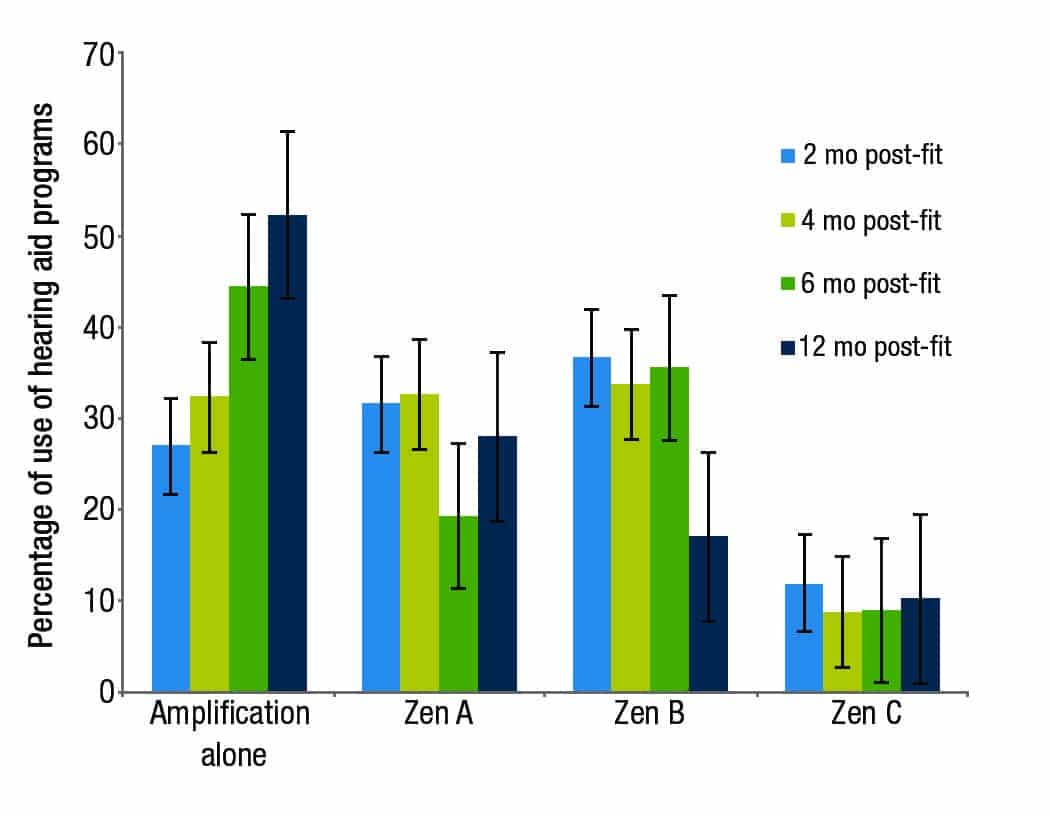
Figure 5. Percentage of use of amplification (Master), Zen A, B, and C at 2, 4, 6, and 12 months. Bars represent standard error.
Figure 5 shows the mean use (in time percentage) of the Zen + programs as well as the amplification alone (the “Master” program) program. Note that, at the 2-month visit, the three Zen + programs were used 73% of the time, but amplification-alone was only used an average of 27% of the time. By the end of the study (ie, 10 months later), however, the combined use of the Zen programs had decreased to 47%, while the amplification-alone usage increased to 53%. A repeated-measures ANOVA indicates a statistically significant increase in the use of amplification over the investigation (p<0.01). Post hoc analysis using a paired-sample test showed a significant increasing in the usage of amplification among all 4 visits (p<0.01).
Keep in mind, however, that the three Zen + programs not only contained fractal tones and/or noise, but also contained amplification (with the exception of two subjects who chose to turn off the microphone in the C program). Therefore, one can confidently say that, as habituation (or resolution of the tinnitus distress) increased, the need for additional sound therapy beyond amplification decreased—though subjects continued to use amplification.
Datalogging also revealed that the Zen A (Aqua + microphone on) and Zen B (Aqua and noise plus microphone on) programs were the most frequently used programs. Despite the unexplained decrease in Zen A use at the 6-month visit, a repeated-measures ANOVA showed no statistically significant differences (p=>0.05) for the use of Zen A over the 4 visits. Conversely, post hoc analysis using a paired-sample testing the use of Zen B showed a statistically significant decrease (p<0.01) at the 12-month visit. This decrease may be related to the fact that subjects had their tinnitus distress reduced over time and no longer felt the need to use fractal tones and noise as frequently as they did during the first 2 months of sound therapy.
The use of Zen C (noise only plus microphone on) was very limited, varying from 9-12% during the 12 months. No statistically significant changes (p>0.05) were seen for the use of Zen C.
Discussion
Two experimental aims were addressed in this investigation. The first was to determine the long-term outcome of the WZT tinnitus management approach. While the effectiveness of an integrated approach like WZT has been repeatedly shown in studies cited earlier, none of those studies looked at the longer-term effects lasting out to 1 year post therapy onset.
The fact that all 19 of the subjects achieved clinically significant improvements when comparing TFI scores from baseline to each of the follow-up visit scores, including those obtained at the 12-month visit, would seem to provide an unequivocal answer to that question. It is of particular importance to note that clinically significant changes were found at the 2-month visit for all of the subjects on the TFI. Moreover, 17 of 19 subjects (91%) had TFI scores suggesting their tinnitus was no longer clinically significant by the conclusion of the 12-month study. Not unexpectedly, there was a trend for the subjects least affected at baseline to also show the least amount of improvement. This tendency has been seen in other studies as well.22,23
Analysis of the second objective—to examine the usage pattern of sound therapy and/or amplification once the patient has achieved a satisfactory resolution or believes habituation has occurred—is somewhat more complicated. One way to approach this issue is to compare the pattern of fractal tone, noise, and amplification-only usage at the 6-month follow-up, since 15 of 19 subjects (79%) achieved clinical resolution of their tinnitus distress (<20 on the TFI) by that visit, to the 12-month follow-up visit. The data showed that the combined use of the three Zen + programs decreased from 56% to 48% (compared to 73% at the 2-month visit), while the use of the amplification-alone (Master) program progressively increased from 44% to 52% (compared to 27% at the 2-month visit). This implies that, as resolution was achieved, subjects tended to utilize the Zen programs, particularly those containing noise (B and C), less frequently while increasing their reliance on amplification-only. The usage of Zen A (fractal tones) decreased somewhat, but this reduction was not statistically significant.
Unfortunately, it is impossible to determine whether the overall use of amplification increased, because even during the 48% of time in which amplification-alone wasn’t being used at the 12-month visit, 17 out of 19 subjects were still utilizing Zen + programs that contained amplification. The exceptions were the 2 subjects who chose to turn off the microphone in Program C at the onset of the project. It is logical to conclude then, that:
1) As habituation (or resolution of the tinnitus distress) increased, the need for additional sound therapy beyond amplification decreased, and
2) Even though subjects had achieved an acceptable resolution of their tinnitus, they still recognized, and in some cases achieved, an even greater appreciation for the benefits received from amplification—either by assisting their hearing or by continuing to minimize their tinnitus distress. This is particularly relevant considering the fact that 17 of the 19 subjects originally presented with primary complaints of tinnitus, rather than hearing difficulty.
One additional point is worth mentioning. As seen in earlier studies, when given the choice between listening to sound therapy containing fractal tones versus programs containing noise, the overwhelming majority (as reflected by comparing usage of Zen A vs Zen C) choose fractal tones. This has been shown in other studies as well,11,12,14 and is likely due to the inherent relaxing qualities of the Zen tones.
Conclusions
On the basis of these results, it can be concluded that:
1) WZT produces a significant decrease in tinnitus distress;
2) The duration of this decrease persists at least out through 12 months;
3) The majority of the reduction occurs within the first 2 months of the treatment; and
4) The relative use of the Zen programs containing noise decreases over time, while the use of amplification alone and/or amplification plus fractal tones increases even after a successful resolution of the tinnitus distress has been achieved.
Results from myriad investigations leave little doubt that WZT is an effective approach to tinnitus management. However, the excellent results obtained in this study are certainly, in part, related to the expertise of the clinicians. It is not realistic to expect the 100% success found in this project to be found in the real world. This point underscores the importance of offering multiple sound therapy options, such as a variety of fractal tone styles and adjustable bandwidth noises, to those patients (approximately 10% in this study) who may prefer acoustic stimuli other than fractal tones.
The inverse relationship between the use of Zen programs versus amplification-alone over time suggests that patients (even those whose primary complaint was tinnitus, rather than hearing loss) perceive a continued benefit for using amplification for improving their hearing, and possibly for tinnitus relief, even post habituation or successful resolution. Further studies are needed to determine the relative contribution of each of the WZT components (including the undisputed importance of counseling), but until these data are available, it seems prudent to utilize the multiple counseling and sound therapy tools offered in an integrated approach like WZT.
Disclosure
Dr Sweetow is a part-time paid consultant for Widex USA.
References
-
Herzfeld M, Enza C, Sweetow R. Clinical trial on the effectiveness of Widex Zen Therapy for tinnitus. Hearing Review. 2014;21(11):24-29. Available at: https://hearingreview.com/2014/10/clinical-trial-effectiveness-widex-zen-therapy-tinnitus
-
Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol. 1996;17:236?40.
-
Jastreboff PJ. The neurophysiological model of tinnitus. In: Snow JB, ed. Tinnitus: Theory and Management. Hamilton, Ontario: BC Decker; 2004:96-107.
-
Searchfield GD, Morrison-Low J, Wise K. Objective identification and attention training for treating tinnitus patients. Progress in Brain Research. 2007;166:441-460.
-
Henry JA, Zaugg TL, Myers PJ, Schechter MA. Using therapeutic sound with progressive audiologic tinnitus management. Trends Amplif. 2008;12(3):188-209.
-
Gold SL, Graw WC, Hu S, Jastreboff PJ. Selection and fitting of noise generators and hearing aids for tinnitus patients. In: Reich GE, Vernon JA, eds. Proceedings of the Fifth International Tinnitus Seminar. Portland, Ore: American Tinnitus Association; 1996:312-314.
-
Jastreboff PJ, Graw WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol. 1996;17:236-240.
-
Wedel HV, Wedel CV, Walger MW. Tinnitus masking with tinnitus-maskers and hearing aids. In: Vernon JA, ed. Tinnitus Treatment and Relief. Needham Heights, Mass: Allyn & Bacon; 1998:187-192.
-
Johnson RM. The masking of tinnitus. In: Vernon JA, ed. Tinnitus Treatment and Relief. Needham Heights, Mass: Allyn & Bacon; 1998:164-186.
-
Khalfa S, Bella SD, Roy M, Peretz I, Lupien SJ. Effects of relaxing music on salivary cortisol level after psychological stress. Ann NY Acad Sci. 2003; 999:374-376.
-
Sweetow RW. The use of fractal tones in tinnitus patient management. Noise and Health. 2013; 15:63;96-100.
-
Sweetow R, Sabes JH. Effects of acoustic stimuli delivered through hearing aids on tinnitus. J Am Acad Audiol. 2010;21:461-473.
-
Kuk F, Peeters H, Lau CL. The efficacy of fractal music employed in hearing aids for tinnitus management. Hearing Review. 2010; 17(10):32-42. Available at: https://hearingreview.com/2010/09/the-efficacy-of-fractal-music-employed-in-hearing-aids-for-tinnitus-management
-
Herzfeld M, Kuk F. A clinician’s experience with using fractal music for tinnitus management. Hearing Review. 2011;18(11):50-55. Available at: https://hearingreview.com/2012/07/a-new-integrated-program-for-tinnitus-patient-management-widex-zen-therapy
-
Sekiya Y, Takahashi M, Kabaya K, Murakami S, Yoshioka M. Using fractal music as sound therapy in TRT treatment. Audiology Online Article #11623 [March 2013]. Available at: http://www.audiologyonline.com
-
Sweetow R. A New Integrated Program for Tinnitus Management. Hearing Review. 2012; 19(7) 20-26. Available at: https://hearingreview.com/2012/07/a-new-integrated-program-for-tinnitus-patient-management-widex-zen-therapy
-
Widex Zen Therapy Manual. Hauppauge, NY: Widex USA. Available at: http://www.widexacademy.com/_reposerver/WZT/Widex_Zen_Therapy_Manual_9%20502%203127%20041.pdf
-
Zubizarreta A, Zubizarreta AF, Jeppesen AK, Caporali SA. Effects of amplification, fractal tones and noise in tinnitus management. Poster presented at: American Academy of Audiology Annual Meeting, Boston, 2012.
-
Skellgaard PH, Kristensen AP, Caporali SA. Effects of counseling, amplification and sound stimulation in tinnitus management. Poster presented at: Tinnitus Research Initiative Annual Meeting, 2013.
-
Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol-Head Neck Surg. 1996; 122:143-148.
-
Meikle MB, Henry JA, Griest SE, Stewart BJ, Abrams HB, McArdle R, Myers PJ, Newman CW, Sandridge S, Turk DC, Folmer RL, Frederick EJ, House JW, Jacobson GP, Kinney SE, Martin WH, Nagler SM, Reich GE, Searchfield G, Sweetow R, Vernon JA. The Tinnitus Functional Index: Development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear. 2012;33(2):153-76.
-
Goddard JC, Berliner K, Luxford WM. Recent experience with the neuromonics tinnitus treatment. Int Tinnitus J. 2009; 15(2):168-73.
-
Newman CW, Sandridge SA. A comparison of benefit and economic value between two sound therapy tinnitus management options. J Am Acad Audiol. 2012. 23(2):126-38.
Robert W. Sweetow, PhD, is Professor of Otolaryngology and former Director of Audiology at the University of California, San Francisco (UCSF); Melodi Fehl, MA, is a Clinical Audiologist and Patti Ramos, AuD, is Director of Audiology and Rehabilitative Services at ENT Associates of South Florida in Boca Raton, Fla.
Correspondence can be addressed to HR or Dr Sweetow at: [email protected]
Original citation for this article: Sweetow, RW, Fehl, M, Ramos, PM. Do tinnitus patients continue to use amplification and sound therapy post habilitation? Hearing Review. 2015;21(3):34.



