Tech Topic: Tinnitus | June 2015 Hearing Review
Sound therapy for the treatment of tinnitus can take many forms; however, all forms of sound therapy are intended to alter the tinnitus perception and reactions for clinical benefit. This article provides a primer on the various approaches to setting the sound therapy signal, including the TRT or TAT/CBT approaches, for patients with and without hearing loss. It also looks at therapy signal alternatives, including the new Ocean Waves Therapy Signals in the Siemens binax devices.
Managing tinnitus has evolved from a highly specialized skill that few treated to something that hearing care professionals (HCPs) must be prepared to address. The steadily increasing number of people with tinnitus—now approximately 1 out of every 10 Americans—has helped drive the need for HCPs to add tinnitus treatment to their armamentarium of services provided. Other drivers include more awareness of the condition than ever, which is tied to a consumer thirst for more information. In fact, according to the Better Hearing Institute, one-third of all hearing loss related online searches are related to tinnitus.
Clearly the pervasiveness of tinnitus necessitates a primer for HCPs looking to add tinnitus services to their practices, or for those wanting a refresher. This paper provides a general guide on how the tinnitus therapy options available in modern hearing aids can be utilized for acoustic therapy.
Although there are many forms of tinnitus, the most common form an HCP will encounter is subjective tinnitus. Subjective tinnitus is the perception of a sound in the ears or in the head with no corresponding external stimuli, most commonly caused by damage to the inner ear.1
There is strong evidence to suggest that acoustic therapy can help mitigate the effects of subjective tinnitus.2 Acoustic therapy can occur in many forms, such as fitting the patient with appropriate amplification, modifying advanced signal processing features for the purpose of tinnitus treatment, or following a formal tinnitus protocol. Let’s examine these in more detail.
Use of Sound Therapy for Tinnitus
Sound therapy for tinnitus is defined as any use of sound intended to alter the tinnitus perception and reactions for clinical benefit. Besides hearing instrument use for tinnitus relief, numerous methods of sound therapy have been used since tinnitus masking was introduced in the 1970s. The two most commonly used are:
1) Total masking: Using an alternative stimulus to cover up (mask) the perceived tinnitus.
2) Partial masking: The addition of an alternative stimulus to reduce the focus of the patient’s subjective tinnitus on both a conscious (psychological level) and unconscious level (central auditory perception).
Both employ the use of broadband noise sound generators, hearing instruments, or combination devices. Sound therapy is thought to provide relief from tinnitus and reduce the emotional consequences of tinnitus.3-5 Additionally, sound therapy may promote habituation to tinnitus by reducing the contrast between the tinnitus and environmental sound. Many researchers have theorized that, if a tinnitus patient is treated early via effective counseling and sound therapy, the effects of the tinnitus can be mitigated before a patient finds him/herself incapacitated by it.
General protocol for setting the therapy signal. Ideally, hearing aids with tinnitus therapy signals should be designed to fit the needs of virtually any established protocol (Figure 1). This flexibility includes the ability to utilize the signal:
- In one or both ears,
- In one or multiple programs,
- At different intensities in each ear,
- At different intensities in each program, and
- With different noise types in each program and/or in each individual ear.
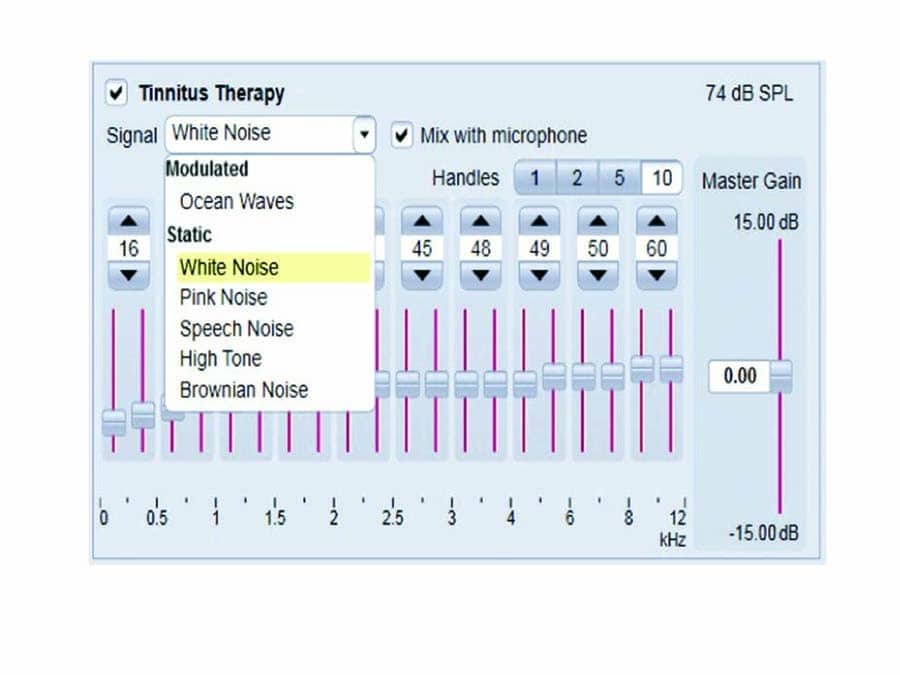
Figure 1. The six noise types as seen in Siemens’ Connexx software.
The HCP may also give the patient a volume control to adjust the therapy signal independent from the hearing aid microphones. The following are suggested protocols for programming the therapy signal according to the more established tinnitus programs, as well as fitting suggestions for those not following a specific tinnitus protocol.
Setting the therapy signals according to Tinnitus Retraining Therapy (TRT).6 TRT uses a precise and individual combination of sound therapy and teaching/demystification/learning about tinnitus and hyperacusis mechanisms, with directions about how to return to normal life without provoking symptoms.
To set the therapy signal according to the TRT protocol, the HCP needs to look for the mixing point: the point where the noise mixes with the tinnitus—without masking it! The HCP chooses one of the therapy sounds and then adjusts in an ascendant technique by utilizing the Master Gain handle (Figure 1). This can be done by first decreasing the Master Gain until the therapy signal is no longer audible to the patient, and then increasing the noise level until the patient says the sound is mixed to tinnitus. To achieve habituation, the noise should not cover the tinnitus. Rather, both sounds should be heard: the therapy sound and the tinnitus itself.
Setting the noiser according to the Tinnitus Activities Treatment (TAT).3-5 TAT is a treatment for the reaction to tinnitus that also uses counseling, sound therapy, and other activities based on Cognitive Behavioral Therapy (CBT). In this case, counseling is structured into four topics:
1) Thoughts and emotions;
2) Hearing and communication;
3) Sleep, and
4) Concentration.
To set the therapy signal according to the TAT protocol, the HCP should also use the ascendant technique and stop when the sound is audible and comfortable for the patient. Many patients report that broadband noise is easier to listen to than their tinnitus. While the goal here is not to achieve total masking or mixing point, it is acceptable to use total masking if the patient prefers it.
For patients with tinnitus and hearing loss. The majority of tinnitus patients seen by HCPs require a combination treatment for both hearing loss and tinnitus. For these patients, it is suggested to first try amplification only. For many patients with tinnitus (and hearing loss), simply wearing hearing aids mitigates the effects of their tinnitus.7
If the amplification of the natural environment isn’t sufficiently reducing the patient’s reaction to tinnitus, a designated hearing instrument program in a mixed mode (microphone+noise) can be activated. Typical set up will include one program with amplification alone and another program with the mixed mode.
For patients that have tinnitus but no hearing loss. When treating tinnitus without hearing loss, a noise-only mode without microphone input is appropriate. In this case, hearing instruments can be used as a simple masker. The amount of noise shaping desired is the primary consideration for these patients, which is often based on the hearing instrument technology level. Here, more economic hearing aid models are appropriate, as they often do not feature the sophisticated amplification algorithms necessary for people with hearing loss.
Therapy Signal Alternatives
Acoustic therapy doesn’t always require a noiser signal in the device or following an established tinnitus treatment protocol. As mentioned above, amplification alone is a common treatment for tinnitus patients,2,8 and is often the starting recommendation by the HCP. However, as hearing instruments have become more sophisticated, less circuit noise has meant much “quieter” hearing aids. Additionally, modern hearing instruments automatically reduce background noise with noise reduction algorithms and directional microphones. Although these advances improve sound quality and comfort for traditional hearing aid wearers, they may be counterproductive for tinnitus patients.
When habituation is the treatment goal, a standard recommendation is to avoid silence.6 However, not all patients are candidates for noise therapy. For these tinnitus sufferers, alternative amplification strategies include:
Frequency shaping. Acoustic therapy with the hearing instrument alone typically involves making environmental sounds more audible for the patient. Some tinnitus patients may prefer a slight increase in soft level gain.
Noise Reduction Modification. In order to use environmental sounds as a natural masking noise for your patient with hearing loss and tinnitus, you many choose to reduce or eliminate some of the noise reduction features. Consider a multi-channel approach of less noise reduction applied in the lower frequencies where “room noise” is typically present. In some cases, it may be advantageous to give the patient a second dedicated program where noise reduction is completely eliminated.
Directional Microphones. HCPs can choose alternative trigger points for the directional microphone modes and varying levels of directionality. A tinnitus wearer may prefer the hearing instrument stay in an omnidirectional mode to amplify more ambient noise when the tinnitus is more intense. This can also be achieved by adding a second program and disabling directional processing.
Streaming accessories. Modern streaming devices like the Siemens easyTek™ connect to virtually any audio device, wirelessly turning a pair of hearing instruments into a personal headset. Patients can now download several apps to the wearer’s smartphone, iPod, tablet, and/or computer and stream relaxation sound files to the hearing instruments. A quick search in Google Play or the Apple App Store for “Tinnitus,” “Relax,” or “Audio” yield several apps that may help complement your tinnitus therapy program.
Counseling
Habituation to tinnitus can take between 12 to 18 months even with appropriate sound therapy. Because of this, many patients return to their HCP feeling discouraged, frustrated, and desperate.
This is why counseling should be an essential part of tinnitus treatment, and is featured prominently in most successful therapy programs such as TRT and TAT. The patient must understand what tinnitus is in order to overcome or avoid the negative associations that inhibit habituation.
Mental health professionals often specialize in CBT, which is commonly used in treating a patient’s psychological response to tinnitus. An HCP may consider a multi-disciplinary approach to tinnitus treatment where the HCP fits and adjusts the hearing instrument for effective sound therapy and provides only the initial tinnitus counseling. Once sound therapy has begun, the mental health professional can provide additional counseling and CBT to further support the emotional well-being of the patient.
Modulated Therapy Signals Tinnitus Therapy
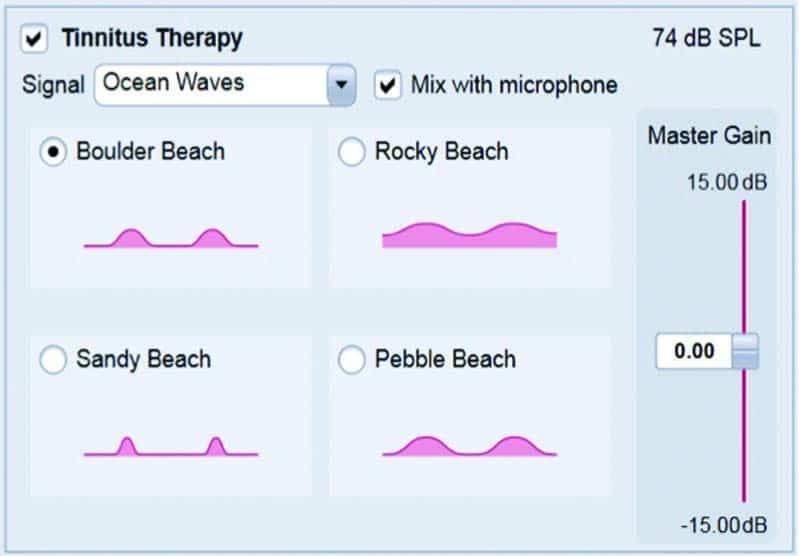
Figure 2. Connexx 7 allows the HCP to customize the modulated therapy signal.
Ocean Waves Therapy Signals was introduced in March 2015 as an expanded feature for all Siemens binax products (Figure 2). These new modulated therapy signals complement the five static therapy noises which can be chosen from a preset or be customized in up to 20 bands by the HCP. The modulating therapy sounds offer built-in “nature sounds” as a tinnitus therapy option. The four modulated signals differ primarily in terms of the intensity and frequency of the modulation, or breaking ocean waves. As an alternative to the more artificial and static therapy noises, these new signals were designed to provide a positive, soothing, and stress-relieving listening experience ideal for tinnitus patients who prefer a more natural therapy signal.
Recent research in tinnitus therapy signals suggests that, although the long-term effects of modulated sounds have yet to be determined, they can be considered for use on a case-by-case basis. As Reavis et al9 pointed out, “in addition to a traditional masking approach using unmodulated pure-tones and white noise, modulated sounds should be used for tinnitus suppression because they may be more effective in reducing hyperactive neural activities associated with tinnitus.”
Conclusion
As discussed in this article, sound therapy for the treatment of tinnitus can take many forms; however, all forms of sound therapy are intended to alter the tinnitus perception and reactions for clinical benefit. Since the patient’s reaction to the configuration of a particular hearing instrument or sound generating device is subjective, there is no right or wrong combination of features to use when it comes to tinnitus treatment. It is recommended that the HCP try different combinations of features at various settings to find what’s right for each patient.
References
-
McFadden D. Tinnitus: Facts, Theories and Treatments. Washington, DC: National Academy Press;1982.
-
Searchfield GD, Kaur M, Martin WH. Hearing aids as an adjunct to counseling: Tinnitus patients who choose amplification do better than those that don’t. Intl J Audiol. 2010;49(8)[Aug]:574-579. doi: 10.3109/14992021003777267.
-
Tyler RS, Gehringer AK, Noble W, Dunn CC, Witt SA, Bardia A. Tinnitus activities treatment. In: Tyler RS, ed. Tinnitus Treatment: Clinical Protocols. New York: Thieme;2006:116–131.
-
Andresson G, Kaldo V. Cognitive-behavior therapy with applied relaxation. In: Tyler RS, ed. Tinnitus Treatment: Clinical Protocols. New York: Thieme;2006:96-115
-
Folmer R, Matin W, Shi Y, Edlefsen L. Tinnitus sound therapy. In: Tyler RS, ed. Tinnitus Treatment: Clinical Protocols. New York: Thieme;2006:176-186.
-
Jastreboff PJ. Phantom auditory perception (tinnitus): Mechanisms of generation and perception. Neurosci Res. 1990;8:221-254.
-
Kochkin S, Tyler R, Born J. MarkeTrak VIII: The prevalence of tinnitus in the United States and the self-reported efficacy of various treatments. Hearing Review. 2011;18(12):10-27. Available at: https://hearingreview.com/2011/11/marketrak-viii-the-prevalence-of-tinnitus-in-the-united-states-and-the-self-reported-efficacy-of-various-treatments
-
Surr RK, Montgomery AA, Mueller HG. Effect of amplification on tinnitus among new hearing aid users. Ear Hear. 1985;6:71-75.
-
Reavis KM, Rothholtz VS, Tang Q, Carroll JA, Djalilian H, Zeng FG. Temporary suppression of tinnitus by modulated sounds. J Assoc Res Otolaryngol [JARO]. 2012 Aug; 13(4): 561–571. doi: 10.1007/s10162-012-0331-6

Leanne Powers, AuD
Leanne Powers, AuD, is an Education Specialist for Sivantos Inc, Piscataway, NJ.
Gisele Munhóes dos Santos, PhD, MD, is an audiologist and Product and Marketing Manager of Sivantos Soluções Auditivas Ltda, São Paulo, Brazil.

Gisele Munhóes dos Santos, PhD, MD
Correspondence can be addressed to: [email protected]
Original citation for this article: Powers L, Munhóes dos Santos G. Acoustic fherapy for the freatment of finnitus: A primer. Hearing Review. 2015;22(6):22.




A great article and overview for those of us who have not fully ventured into Tinnitus treatments. Feeling inadequate we HCPs may be the reason many tinnitus sufferers do not have this treatment suggested. Thank you for the push in the right direction. I will drop my perfectionism and recommend TAT regardless.