A number of studies have shown that it may not be possible to predict directional benefit. This study suggests that it is somewhat possible when looking at an individual’s threshold below 500 Hz and 1000 Hz, benefit scores on certain subscales of the APHAB, and venting needs.
Directional microphones improve the signal-to-noise ratio (SNR) of the listening environment.1-3 The magnitude of the improvement—the difference in SNR between performance with an omnidirectional microphone and a directional microphone, or directional benefit—was shown to be dependent on the reverberation characteristics of the listening environments,4,5 number of competing noise sources in the background and azimuths of the noise sources,6,7 and other factors in the environment.8 On the other hand, it is less clear if the audiometric characteristics of the wearers may affect the magnitude of the directional benefit9,10 or if the amount of directional benefits seen in the clinic can be extrapolated to daily use of the device.7,11
Killion et al.12 played the recorded output of a switchable directional in-the-ear (ITE) hearing aid to listeners with normal hearing and those with a mild-to-moderate hearing loss. The average listener received 4-5 dB SNR improvement in the directional mode over the omnidirectional mode. However, the authors also noted that the improvement was greater in listeners with a sloping hearing loss (6.3 dB) than those with a flat loss or normal hearing (around 4-5 dB). Killion & Christensen13 attributed this difference to the interaction between the directivity index of the microphone (6.2 dB below 1600 Hz versus 3.4 dB above 1600 Hz) and the listeners’ higher SNR loss in the higher frequencies. Those with a flat loss were unable to use the low-frequency information where the directivity was the greatest.
On the other hand, Ricketts & Mueller10 examined the directional benefit data of 80 subjects (from 3 separate experiments) to determine if the slope of the audiogram, the magnitude of the high-frequency hearing loss, and the SNR loss of the individual would correlate with directional benefit. In contrast to Killion et al’s observations,12 no correlation was found between directional benefit and audiometric variables. Ricketts & Mueller recommended that “…until contrary evidence emerges, clinicians should consider the use of directional amplification for patients regardless of audiogram slope, degree of high frequency hearing loss, or omnidirectional HINT thresholds.”10
Recently, Jespersen & Olsen9 examined the SNR required on the Dantale II Hagerman sentences14 in three groups of listeners with a mild (PTA < 40 dB HL, n= 12), moderate (PTA < 55 dB HL, n=10), and moderate-to-severe loss (PTA < 90 dB HL, n=10) using an adaptive directional BTE hearing aid. Although the SNR in the omnidirectional mode and the directional mode correlated significantly with the PTA, directional benefit was not correlated with the PTA or with the SNR obtained for the omnidirectional microphone mode. These authors concluded that “…predictability of directional benefit is to be found from the characteristics of the listening situations encountered by the hearing impaired, rather than from audiological factors.”9
Although the conclusions from Ricketts & Mueller10 and Jespersen & Olsen9 are probably valid for their designs, two issues remained that may have biased the observations and conclusions relative to the independence of directional benefit from audiometric variables. In many studies of directional hearing aids, testing was done with minimal vent diameter (<1-1.5 mm) or no vents and on listeners with primarily a mild-to-moderate degree of hearing loss. Presumably, minimal or no venting was used in order to preserve the directivity of the directional microphones.
In the real world, however, people with a sloping hearing loss are frequently prescribed hearing aids (or earmolds) with more than a pressure vent. One reason is to reduce the occlusion effect (OE) when the wearer speaks or vocalizes.15 On average, the occlusion effect results in an increase in output below 500 Hz by as much as 20 dB.16 For individuals with normal-to-mild hearing loss in the low frequencies, this increased gain in the low frequencies could be especially bothersome because it is significantly above their hearing thresholds. To decrease the OE that has a shell origin, vent diameters are typically increased. Revit,16 Mueller,17 and Westermann18 suggested that vents must have at least a 2-mm diameter in order to reduce the majority of the OE.
In addition to increasing the risk of feedback and reducing the amount of gain in the low frequencies as the vent diameter is increased, the directivity index (DI) of a directional hearing aid also decreases as the vent diameter increases. Ricketts6 measured the polar directivity patterns of 12 directional hearing aids across 4 vent conditions in both the omnidirectional and directional modes. His results showed a significant decrease in the DI below 1000 Hz. Similar findings on the effect of vents were reported by other researchers.19
The use of no vent or a pressure vent in directional hearing aid testing has the advantage of maximizing the potential directional benefit of a directional microphone during the clinical evaluation; however, for those with a sloping hearing loss, it may exaggerate the directional benefit received once their hearing aids (or earmolds) are adjusted to minimize the occlusion effect. Consequently, the conclusion that directional benefit is independent of hearing loss configurations (and degrees) may be limited to specific experimental conditions and may not be valid in the real world.
There is a second issue that may affect the ability to draw broad generalizations about this data. The majority of the listeners reported in the studies had a mild-to-moderate sloping sensorineural hearing loss. Restricting the degree (or range) of hearing loss is likely to alter the magnitude of the estimated ensemble correlation coefficient.20 For example, if you wish to examine the correlation between hearing loss at 500 Hz and word recognition scores, you need to include subjects with various degrees of hearing loss at 500 Hz instead of restricting hearing loss from 20-40 dB HL. This truncated range (eg, compared to 10-80 dB HL, for example) could weaken the correlation. Furthermore, it limits the generalizability of the data to only subjects with a mild-to-moderate degree of hearing loss.
A third problem with generalizing the magnitude of directional benefit in the real world is that some signal processing features may interact with the directional microphones. For example, many digital hearing aids today have noise reduction algorithms—some of which may enhance or compromise the benefits of the directional microphone. Yet, many of these algorithms were inactive during the clinical evaluation of the directional microphone. In the real world, these algorithms are active (along with the directional microphone) to shape the input sounds and affect wearer satisfaction with the hearing aids. That is, the magnitude of the directional benefit may be specific to the hearing aids under evaluation.
These considerations prompted us to reexamine the correlations between audiometric variables and directional benefits using listeners with various hearing loss configurations fit with more appropriate vent diameters for real-world hearing aid use.
Study Method
Study participants. The first 17 volunteers seen at Widex’s research office were included in this study. These individuals had various degrees and configurations of sensorineural hearing loss that were symmetrical between ears (±10 dB). Of the study participants, 10 had worn hearing aids before, and 7 were first-time wearers. Thirteen of the participants were fit with in-the-canal (ITC) hearing aids, 1 was fit with in-the-ear (ITE) aids, and 3 were fit with behind-the ear (BTE) aids. Figure 1 shows the averaged individual audiograms for the 17 participants. Although the subjects were paid for their participation, none were informed about the nature of the study or the identity of the study hearing aids.

Hearing aids. Binaural Widex Senso Diva hearing aids were used in the study. This is a 15-channel digital hearing aid that uses primarily slow-acting compression with a low compression threshold at 0 dB HL. This hearing aid also has a noise reduction algorithm that uses level distribution function for noise identification.21 Graded gain reduction occurs only when the “noise” is above a conversational level. Depending on the input level, the effectiveness of this algorithm may be affected by the use of a directional microphone (compared to an omnidirectional microphone). There is also an active feedback cancellation algorithm that minimizes the occurrence of feedback by canceling the feedback signal.22 This is designed to allow for more usable gain before feedback and should not affect the performance of the directional microphone. Lastly, there is an occlusion manager that is designed to minimize occlusion complaints related to the amplifier.23 This algorithm also should not impact the use of the directional microphone. These algorithms were active during the data collection and daily use of the study hearing aids.
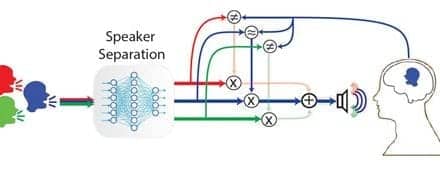
The fully adaptive directional microphone used in the study hearing aid receives input from two omnidirectional microphones. The key features of this microphone system are an OptiMic that ensures identical sensitivity and phase characteristics of the two microphones at all times; a Noise Classifier that decides if the input is wind noise, circuit noise, or typical environmental sounds (i.e., speech and other sounds); a Signal-to-Noise Optimizer that determines the optimal SNR of the listening environment; and a Beamformer that adaptively changes the polar pattern from an omnidirectional pattern to a cardioid, hypercardioid, supercardioid, bidirectional, or any patterns in between while compensating for low-frequency sensitivity. To minimize the loss of audibility for sounds from the sides and back, a 5-10 s switching time was used for the hearing aid to switch from an omnidirectional mode to the appropriate directional pattern. The in-situ DI of the directional microphone was about 4-6 dB across frequencies for the ITC/ITE model and slightly lower for the BTE (4-5 dB). A detailed description of the rationale and mechanism of this microphone can be found in Kuk et al.24
Test materials and conditions. Sentences from the Hearing In Noise Test (HINT)25 were used to estimate the SNR required for 50% recognition. A continuous party noise recorded at the Old Copenhagen Stock Exchange with babble and music in the background26 was used as the competing stimulus. The noise level was fixed at 68 dB SPL(A) while the level of the speech signal was adaptively adjusted. The speech material was presented in the front (ie, 0°) while the uncorrelated noise was presented to the sides and rear (ie, 90°, 180°, and 270°). Normative data on 20 normal-hearing participants obtained under the identical test conditions showed a mean SNR requirement of 0 dB with a test-retest variability of less than 2 dB. The APHAB questionnaire27 was used as an evaluation of the participants’ performance with the study hearing aids during their “real-world” use.
Procedure. All testing was conducted in a double-wall sound-treated booth (Industrial Acoustics) that has internal dimensions of 10’ x 10’ x 6’6”. During speech testing, participants were seated 1 meter from each of the test loudspeakers (Cerwin-Vega). During the first session, the unaided HINT and APHAB performance was measured and the appropriate hearing aids were ordered.
Participants were fit with binaural study hearing aids following the same guidelines. First, the appropriate in-situ orientation of the hearing aids was ensured. Afterwards, the vent diameter on the study hearing aids was specified using the participants’ hearing loss at 500 Hz as a guideline. Specifically, a parallel vent with a 2.0-2.5 mm diameter was installed for a hearing loss less than 30 dB HL at 500 Hz. As the hearing loss at 500 Hz increased, vent diameter decreased 0.5 mm for every 10 dB increase in thresholds. The participants’ in-situ hearing thresholds at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz were then measured to specify gain targets at various input levels. A feedback test was performed afterwards to ensure sufficient gain and optimal estimation of the feedback path.
Participants wore the study hearing aids for 2 weeks before returning for a fine-tuning session. The hearing aids were left in the default automatic adaptive directional microphone mode. The study participants returned monthly for speech testing in noise. Data collected at the fourth or last visit were reported. Study participants also returned the completed aided portion of the APHAB questionnaire at the last visit.
Study Results
Performance on the HINT. Figure 2 shows the average SNR for 50% correct on the HINT for the unaided condition (Unaid), the study hearing aid in the omnidirectional mode (Omni), and the study hearing aid in the adaptive directional mode (Dir). The average SNR was 9.35 dB for the unaided mode, 5.11 dB for the omni-directional mode, and -0.79 dB for the directional mode. Compared to the unaided condition, the study hearing aid improved the SNR by 4.24 dB in the omnidirectional mode and 10.14 dB in the directional mode. The average SNR improvement by the directional microphone was 5.9 dB. A one-factor repeated measure analysis of variance (ANOVA) test showed that the SNR differences among the three test conditions were significant (F[2,32] = 44, p < 0.001). Post-hoc Tukey-HSD test showed that the SNR achieved in each condition was significantly different from each other (p < 0.001).
Correlations between HINT scores and audiometric variables. Table 1 summarizes the correlation coefficients between HINT scores and the audiometric and demographic variables. HINT performance was measured without any hearing aids (HINTUN), with the study hearing aids in the omnidirectional mode (HINTOM), and adaptive directional mode (HINTLOC). The improvement in SNR (HINTIMP) with the automatic adaptive directional microphone (versus the omnidirectional mode) was also included. The demographic variables included the participants’ age, gender, years of hearing aid use, speech recognition score on the W-22 word test obtained under headphones in quiet, and the diameter (in millimeters) of the vent used during the study. The audiometric variables included participants’ hearing loss measured at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz, the pure-tone average at 500 Hz, 1000 Hz, and 2000 Hz, the high-frequency hearing loss (average at 2000 Hz, 3000 Hz, and 4000 Hz), and the slope of the audiogram (((HL500 Hz – (average loss at 2000 Hz, 3000 Hz, and 4000 Hz)) ÷ 2.5 octave), as suggested in Ricketts & Mueller.10

Audiometric variables on hearing levels in the high frequencies such as HL3000, HL4000, and average high-frequency loss (HFA) did not show significant correlation with the HINT scores obtained in any microphone conditions. HINT scores obtained with the omnidirectional microphone (HINTOM) correlated significantly with HL500 (r=0.74, p=0.001), PTA (r=0.60, p=0.01), and slope (r=0.60, p=0.01). This suggests that higher HINT scores (or poorer speech understanding in noise) are associated with more hearing loss in the low-to-mid frequencies. HINT scores obtained with the adaptive directional microphone (HINTLOC) did not correlate with any audiometric variables; however, many of these variables correlated significantly with HINTIMP scores. For example, a correlation coefficient of r = 0.792 (p =0.0001) was obtained between HINTIMP and pure-tone average (PTA) and slope of audiogram. The correlation coefficients (r) were 0.788 (p=0.0001) with HL500 and 0.825 (p=0.0001) with HL1000. These results showed that subjects with more hearing loss between 500-1000 Hz received more directional benefit than those with less hearing loss at these frequencies.
Demographic variables such as age, gender, years of hearing aid use did not correlate significantly with HINT scores obtained in any conditions. On the other hand, vent size correlated significantly with HINTUN (r= -0.71, p = .001), HINTOM (r = – 0.69, p =.002), and HINTIMP (r = -0.74, p=.001), but not with HINTLOC (r = -0.26, p=.311). The negative correlation between vent diameters and HINT scores suggests that higher HINTOM and HINTUN scores were associated with vents of smaller diameters. Because vent diameters were predetermined by the degree of hearing loss at 500 Hz, these correlations reflected poorer speech in noise performance (ie, higher HINT scores) as hearing loss increased. In the same vein, the negative correlation between vent diameter and HINTIMP suggests that participants who used a larger vent diameter (and, thus, had less hearing loss) received less SNR improvement from the use of the directional microphone over the use of the omnidirectional microphone. The lack of a significant correlation between HINTLOC and vent diameter suggests that performance of the study hearing aids in the directional mode was similar among participants.
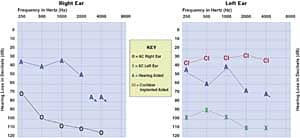
Figure 3 is a scatter-plot summarizing the individual HINT scores for the unaided, aided-omni, and aided-directional conditions. Each symbol represents the data of one participant under one of the test conditions. Additionally, the regression lines and the R2 are included. The slopes of the regression lines were estimated to be 0.29 (ie, an increase in SNR of 2.9 dB for every 10 dB increase in hearing loss) for the unaided condition and 0.16 (ie, an increase in SNR requirement of 1.6 dB for every 10 dB increase in hearing loss at 500 Hz) for the omnidirectional microphone condition. On the other hand, the HINT scores obtained in the adaptive directional mode did not seem to depend on the hearing loss of the participants because the average participant required the same SNR of 0 dB to -1 dB in the directional mode. This is consistent with the observed lack of significant correlation between HL500 and the adaptive directional mode (HINTLOC).
The “vertical distance” in Figure 3 between the regression lines obtained for the omnidirectional microphone (long and short dashed line) and the directional microphone (dotted line) reflects the directional benefit as a function of hearing loss at 500 Hz. Although not displayed in Figure 3, one can visualize that the separation between the dashed line and the dotted line increased as the hearing loss at 500 Hz increased. Thus, directional benefit increased with hearing loss at 500 Hz (and 1000 Hz also, not shown).
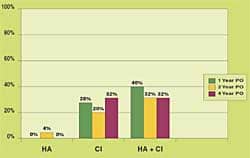
Correlations between HINT scores and APHAB scores. Figure 4 summarizes the average difficulty score for both the aided (automatic adaptive directional mode) and unaided conditions for each of the subscales on the APHAB questionnaire. The difference between the aided and the unaided difficulty reflects the real-world benefit of the study hearing aids in their default automatic adaptive directional mode. With the exception of the AV subscale, benefit scores varied between 30%-40% across subscales. A two-factor repeated measure ANOVA was used to test the effect of hearing aid condition (unaided and aided) and each subscale on the APHAB. The results confirmed a significant overall interaction of the two factors (F[4,60] = 17.59, p < 0.001) and significance for each of the two factors (hearing aid: F[1,15] = 41.78, p < 0.001; APHAB subscale: F[4, 60] = 14.53, p < 0.001). Post-hoc paired t-tests confirmed that the noted difference seen on all but the AV subscale was statistically significant (p < 0.05).

Table 2 summarizes the correlation coefficients between the HINT scores obtained in different test conditions (unaided, omnidirectional, directional, and benefit) and scores on the APHAB questionnaire (unaided, aided, and benefit). HINT scores obtained in all but the adaptive directional mode (HINTLOC) correlated significantly (p < 0.05) with unaided APHAB scores on all but the aversiveness of sound (AV) subscale. This suggests that the HINT scores obtained in the unaided and aided conditions with the omnidirectional microphone may predict the amount of real-world difficulty without a hearing aid.
In the aided condition with the default adaptive microphone, significant correlations (p < 0.05) were seen between APHAB background noise, reverberation, and global subscales, and the HINT obtained in all (ie, HINTUN, HINTOM, HINTIMP) but the adaptive directional mode (exception: background noise subscale and HINTLOC). This suggests that participants who reported more difficulty in the aided BN and RV subscales also tended to require a higher SNR on the HINT when they were unaided and aided with an omnidirectional microphone. It was also true when the participants wore the adaptive directional microphone for the Background Noise subscale. The significant correlation between HINTIMP and the APHAB subscale scores suggests that those individuals who had more difficulty in noise and reverberation—even in the aided directional condition—tended to receive more SNR improvement (directional benefit) than those with less difficulty.
On the other hand, only the APHAB benefit scores on the Ease of Communication (EC) and Global (GL) subscales correlated significantly with the HINT scores measured in the unaided (HINTUN), aided with omnidirectional microphone (HINTOM), and the directional benefit (HINTIMP). This suggests that those who received the most overall benefit and benefit in quiet situations (EC and GL subscales) from the study hearing aid also had higher HINT scores (or poorer speech recognition in noise) in the unaided (HINTUN) or omni-mic (HINTOM) conditions. However, these were also the individuals who received the most improvement in HINT scores (HINTIMP).
In summary, those who required a high SNR on the HINT also reported more difficulties on the APHAB. However, those who reported more difficulties (and required a higher SNR) also reported more directional benefits.
Discussion
The present study demonstrated that the magnitude of the directional benefits may be compromised by real-world fitting constraints, such as the vent diameter used on the hearing aid and additional processing features on the hearing aids. It also showed that directional benefits correlate with the listeners’ hearing thresholds at 500 Hz (and 1000 Hz) and benefit scores measured on some subscales of the APHAB questionnaire. These observations stress the importance of subject sampling and hearing aid variables that may affect the generalization of results from laboratory studies.
There were several designs in this study that were markedly different from the studies cited in the introduction of this article. First, listeners with varied hearing loss configurations and degrees (eg, precipitous hearing loss and severe hearing loss) were included in this study. These individuals introduced more differences in their speech recognition in noise ability and responsiveness to different types of signal processing such as noise reduction. Statistically, this increased dispersion of the range of subjects may have resulted in a better estimate of the relationship between directional benefits and audiometric variables.
Because of the inclusion of listeners with a normal-to-mild hearing loss in the low frequencies, the choice of an “appropriate” vent diameter became critical. This study used vent diameters that were as wide as 2.5 mm for participants with good low-frequency hearing. The effect of an increase in vent diameter is a decrease in the directivity index below 1000 Hz. Indeed, Mueller & Wesselkamp18 indicated that a 2 mm vent will decrease the DI by 2.3 from the occluded condition. This suggests that the participants with essentially normal hearing at 500 Hz may only receive at most 2-4 dB of directional benefit (instead of the typical 4-6 dB) from the use of the directional microphone. On the other hand, this group of listeners would have less SNR loss than those with more hearing loss (as seen in the omni mic mode). Those with a more severe hearing loss received more SNR benefit from the study hearing aids, despite having a poorer SNR loss. These two factors probably complemented each other to result in similar performance on the HINT for all participants in the adaptive directional mode.
A third difference may stem from the processing used in the different hearing aids. Many of these studies10-12 evaluated directional benefit in single-channel or two-channel compression hearing aids. Although Jespersen & Olsen9 used a 14-channel digital hearing aid, special signal processing like the noise reduction algorithm was deactivated during the study. One may assume that this was done to isolate the directional effect. On the other hand, directional microphones are increasingly used in conjunction with hearing aids utilizing various types and levels of signal processing (such as multi-channel and noise reduction) in the real world. These algorithms may interact with the actions of the directional microphone to further enhance (or reduce) the potential SNR benefits offered by the specific hearing aid. If so, one cannot conclude on the magnitude of the total SNR benefit without specifying the type of processing to which the directional microphone is coupled.
Because the noise reduction is active in both the omnidirectional and directional modes, one would expect its net effect to be zero. That is, the regression line for the omnidirectional microphone should be parallel to that of the directional microphone if all the participants received the expected 4-6 dB SNR improvement. Yet, in this case, the regression line for the directional mode was “flat.” This suggests that those with a more severe loss received more benefit from the study hearing aid than those with a mild-to-moderate hearing loss. Perhaps, for this group of hearing aid wearers, the reduction in physical intensity of the inputs from the combined actions of the directional microphone and the noise reduction algorithm resulted in more overall SNR improvement than simply adding the SNR advantages of both features. This possibility of interactions among signal processing strategies and wearer characteristics needs further examination.
In addition to the noise reduction algorithm, this study hearing aid also has a low compression threshold and an automatic, adaptive directional microphone. These two features were also drastically different from the hearing aids reported in the previous studies in that some of the limitations of a directional microphone, such as a potential loss of audibility for soft sounds, may be minimized. This probably did not affect the results on the HINT, but it could have contributed to performance on the APHAB. Perhaps that is why Walden et al.28 found little correlation between ratings on the real-world questionnaire and SNR provided by a fixed directional microphone, whereas this study showed significant correlation between the HINT scores obtained in all conditions and the aided APHAB on the Background Noise subscale.
Directional Benefit and Fitting Implications
This study suggests that directional benefits are, to some extent, predictable from the hearing loss of the potential wearers. Listeners with a normal-to-mild hearing loss in the low-to-mid frequencies may not receive as much directional benefits as those with a moderate degree of hearing loss in these frequencies. However, the reason is not because they have a mild hearing loss; it is due to the use of vent diameters that may compromise the directivity index of the microphone in the low-to-mid frequencies.
The observed directional benefits for those with near-normal hearing or mild hearing loss may improve if pressure vents were used in this study instead. On the other hand, vents are used for the purpose of minimizing the occlusion effect, especially for first-time hearing aid wearers with a mild hearing loss. It is an important clinical decision if one should maximize the directional benefit by using a small vent diameter (and potentially aggravating the occlusion effect) or minimize the occlusion problem by increasing the vent diameter (and risk losing some of the directional benefit of a directional microphone). Because the participants with the mildest loss in this study received about 2 dB SNR improvement and that they may not have as much SNR loss (as those with a more severe loss) to begin with, one may opt to accept a compromised SNR improvement by using a vent diameter that is large enough to result in acceptable voice quality.
Another implication is that the choice of study participants and the manner in which the study hearing aids are fit have significant impact on the generalizability of the results to daily fittings. The conclusions from previous studies (ie, independence of directional benefits from audiometric variables) are valid only for mild-to-moderate hearing losses fit with a pressure vent. It may not be true for other configurations and degrees of hearing losses. In this study, inclusion of participants with a more severe loss and the use of the noise reduction feature may add to the directional benefit while the use of participants with a milder loss (along with the use of 2-2.5 mm vent diameter) may reduce the SNR potential. Like the limitations in other studies, these observations (and conclusions) are specific to the hearing aids used in the current study and may not be generalized.
Should one include subjects with diverse backgrounds in conducting clinical research? In correlation analysis, it is a requirement that the dispersions of both variables are similar in order to fairly estimate the standard error of estimate. From that perspective, it is crucial that subject sampling be representative of real-life occurrence—the ethnicity, gender, degree of hearing loss, as well as the configuration of hearing loss and cognitive abilities—if one were to generalize the results to daily applications. On the other hand, such a demand is almost impossible to meet because of the cost and scarcity of potential participants who meet all the criteria. However, researchers should encourage as much diversity that is representative of the general population during subject recruitment, and be specific in the conclusions on the generalizability of the findings. Readers should also be careful not to over-interpret the results as well.
| This article was submitted to HR by Francis Kuk, PhD, director of audiology, and Denise Keenan, MA, assistant research audiologist at the Widex Office of Research in Clinical Amplification-USA, Lisle, Ill; and Carl Ludvigsen, MS, manager of audiological research at Widex A/S, Vaerloese, Denmark. |
References
1. Amlani A. Efficacy of directional microphone hearing aids: a meta-analytic perspective. J Am Acad Audiol. 2001;12(4):202-214.
2. Ricketts T. Directional Hearing Aids. Trends Amplif. 2001;5(4):139-176.
3. Valente M. Use of microphone technology to improve user performance in noise. Trends Amplif. 1999;4(3):112-135.
4. Hawkins D, Yacullo W. Signal-to-noise ratio advantage of binaural hearing aids and directional microphones under different levels of reverberation. J Speech Hear Disord. 1984;49(3):278-286.
5. Ricketts T, Dhar S. Comparison of performance across three directional hearing aids. J Am Acad Audiol. 1999;10(4):180-189.
6. Ricketts T. Directivity quantification in hearing aids: fitting and measurement effects. Ear Hear. 2000;21(1):45-58.
7. Valente M, Mispagel K. Performance of an automatic adaptive dual microphone ITC digital hearing aid. Hearing Review. 2004;11(2):42-46,71.
8. Surr R, Walden B, Cord M, Olson L. Influence of environmental factors on hearing aid microphone preference. J Am Acad Audiol. 2002;13(6):308-322.
9. Jespersen C, Olsen S. Does directional benefit vary systematically with omnidirectional performance? Hearing Review. 2003;10(11):16-24.
10. Ricketts T, Mueller G. Predicting directional hearing aid benefit for individual listeners. J Am Acad Audiol. 2000;11(10):561-569.
11. Walden B, Surr R, Cord M, Edwards B, Olson L. Comparison of benefits provided by different hearing aid technologies. J Am Acad Audiol. 2000; 11(10):540-560.
12. Killion M, Schulein R, Christensen L, Fabry D, Revit L, Niquette P, Chung K. Real-world performance of an ITE directional microphone. Hear Jour. 1998;51(4):24-38.
13. Killion M, Christensen L. The case of the missing dots: AI and SNR loss. Hear Jour. 1998;51(5):32-47.
14. Wagener K, Josvassen J, Ardenkjaer R. Design, optimization, and evaluation of a Danish sentence test in noise. Intl J Audiol. 2003;42(1):10-17.
15. Kampe S, Wynne M. The influence of venting on the occlusion effect. Hear Jour. 1996;49(4):59-66.
16. Revit L. Two techniques for dealing with the occlusion effect. Hear Instrum. 1992;43(12):16-18.
17. Mueller G. CIC hearing aids: What is their impact on the occlusion effect? Hear Jour. 1994;47(11):29-35.
18. Westermann S. The occlusion effect. Hear Instrum. 1987;38(6):43.
19. Mueller G, Wesselkamp M. Ten commonly asked questions about directional microphone fittings. In: Kochkin S, Strom KE, eds. High Performance Hearing Solutions, Vol 3: Hearing In Noise. Hearing Review. 1999;6(1)[Suppl]:26-30.
20. Nunnally J, Jr. Introduction to Psychological Measurement. New York: McGraw-Hill; 1970:95-96.
21. Kuk F, Ludvigsen C, Paludan-Muller C. Improving hearing aid performance in noise: Challenges and strategies. Hear Jour. 2002;55(4):34-46.
22. Kuk F, Ludvigsen C, Kaulberg T. Understanding feedback and digital feedback cancellation strategies. Hearing Review. 2002;9(2):36-43.
23. Kuk F, Ludvigsen C. Ampclusion II: A 5-step approach to remediation. Hearing Review. 2002;9(9):34-43.
24. Kuk F, Baekgaard L, Ludvigsen C. Using digital signal processing to enhance the performance of dual microphones. Hear Jour. 2002;55(1):35-45.
25. Nilsson M, Soli S, Sullivan J. Development of the Hearing in Noise Test for the measurement of speech reception thresholds in quiet and in noise. J Acoust Soc Am. 1994;95(2):1085-1099.
26. Valente M, Fabry D, Potts L, Sandlin R. Comparing the performance of the Widex SENSO digital hearing aid with analog hearing aids. J Am Acad Audiol. 1998;9(5):342-360.
27. Cox R, Alexander G. The abbreviated profile of hearing aid benefit. Ear Hear. 1995;16(2):176-186.
28. Walden B, Surr R, Cord M. Real-world performance of directional microphone hearing aids. Hear Jour. 2003;56(11):40-47.