
SPECIAL ISSUE: Unilateral Hearing Loss | October 2019 Hearing Review
A literature review on unilateral hearing loss and the effectiveness of CROS/BiCROS fittings
Unilateral and asymmetric hearing loss are some of the most poorly understood—and sometimes confusing—audiological conditions commonly encountered in a hearing care practice. This article looks at the various forms of unilateral loss and reviews the various treatment methods with particular emphasis on CROS and BiCROS hearing aid fittings.
The terms single-sided deafness (SSD), asymmetric sensorineural hearing loss (A-SNHL), unilateral sensorineural hearing loss (U-SNHL), and sudden sensorineural hearing loss (S-SNHL) have similar and sometimes confusing or over-lapping meanings. In this article, we’ll explore these terms, as well as the hearing aid fittings and outcomes associated with them.
Terminology
The terminology used to describe worse hearing in one ear is highly variable. Perusal of the literature may leave one confused as to how to accurately describe this type of hearing loss. Use of the various terms and their associated criteria differs by the user and/or their preference.
In medical settings, physicians and surgeons are primarily concerned with determining the etiology of hearing loss and whether it can be treated medically or surgically. In research studies, classification of hearing loss may be accomplished for the purpose of defining inclusion and exclusion criteria for study participation. Audiologists may characterize hearing loss based upon the usability of the auditory system for communication function and alleviation of perceived impairment. The terminology and associated definition that one uses is likely impacted by their training and their role in supporting people with these atypical hearing losses. The review of recent literature which follows illustrates the complexity inherent in defining SSD, A-SNHL, U-SNHL, and S-SNHL.
In a recent paper, Lipschitz et al1 defined SSD as a unilateral profound hearing loss in the presence of a contralateral normal hearing ear. They defined A-SNHL as the worse hearing ear having a profound hearing loss, while the better hearing ear has a mild-moderate hearing loss. Bowers2 reports U-SNHL indicates one ear has normal thresholds, while the impaired ear has any degree of hearing loss. Bowers notes SSD is a subset of U-SNHL in which the impaired ear has no usable hearing.
Although some definitions pivot on severity or onset, these factors can be difficult to define. Severity indicates degree of hearing loss in decibels, not clarity of sound, nor the ability to listen, localize, or attend. That is, some people with U-SNHL may have hearing loss which is severe or profound regarding their pure-tone average (PTA), yet they may hear clearly when sound is comfortably loud. Others with the same degree of hearing loss may be unable to repeat words, yet they may be able to use the sound perceived in that ear to locate sound.
Likewise, the term SSD can be problematic. The word “deaf” (as in “single sided deafness”) indicates a hearing loss of 91 dB HL or greater. Thus, hearing sounds at normal conversational loudness levels is precluded. Yet, this same ear may hear extraordinarily loud sounds (ie, the ear hears, but requires very loud sound, versus completely non- functional hearing). Further, SSD has been used to describe sudden onset hearing losses of varying degrees.
With respect to degree of hearing loss, in practice, SSD, A-SNHL, U-SNHL, and S-SNHL may range from mild to profound. Further complicating the issue is that beyond the degree of hearing loss as measured in decibels, word recognition scores (WRS) may range from 0 to 100%. Van de Heyning and colleagues3 define A-SNHL or SSD consistent with previous definitions (eg, Vincent et al, 20154] and based on the four-frequency PTA of 0.5, 1, 2, and 4 kHz. They state SSD involves a poorer ear with a PTA greater than or equal to 70 dB HL, and a better ear PTA of 30 dB HL or better (see their Table 1).3 Whereas A-SNHL requires a poorer ear PTA greater than or equal to 70 dB HL, and the better ear PTA presents between 30-55 dB HL.
As this article concerns the non-medical and non-surgical treatment options for permanent hearing losses, we will conceptualize UHL/AHL/SSD as a hearing loss in which one ear is significantly worse than the other, affecting patient function in a negative way and for which binaural amplification has proven to be inappropriate or insufficiently beneficial. It is these cases that alternative treatment options should be considered.
Etiology and Epidemiology
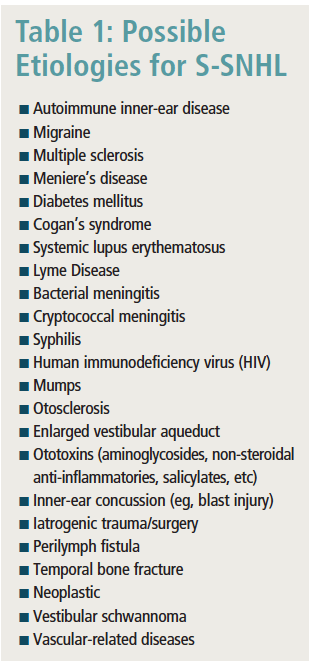
The timing of the occurrence of UHL/AHL/SSD will likely impact the role that this hearing loss has on patient function. Onset of UHL/AHL/SSD is often considered to be “sudden.” With regard to S-SNHL, 98% of all cases are unilateral and the possible etiologies are vast, including but not limited to those listed in Table 1. Kuhn et al5 point out that a specific etiology is identified in fewer than half of all cases. Fal et al6 note that, if S-SNHL is defined as a hearing loss within 72 hours of 30 ?dB or more hearing loss across at least 3 neighboring frequencies, then S-SNHL occurs approximately 10 times per 100,000 people.6 It should be emphasized that S-SNHL (in one or both ears) is, in many respects, one of the few “emergencies of the ear” encountered in a hearing care practice and often warrants an immediate/urgent medical referral.7
Reported rates of UHL/AHL/SSD vary widely—likely due to differences in definition and measurement of the disorder. Unilateral congenital hearing loss is relatively rare (Bowers2 notes that 1 per 100,000 newborns has U-SNHL at birth), yet by age 3, 3% of children (3,000 per 100,000) may have developed USNHL. Hear-It.org8 reports more than 60,000 people in the United States develop unilateral hearing loss annually. Meehan et al9 estimate up to 10% of the world’s population has single-sided deafness, unilateral hearing loss, or a significant asymmetrical hearing impairment.
Associated Hearing and Listening Problems
If we only consider the impact of UHL/AHL/SSD on audibility of speech, we might make the mistake of assuming that these conditions result in a minimal or mild impairment, as speech can still be perceived by the better ear. However, the effect is significant, as shown by Galloway and colleagues10 who in the April 2019 Hearing Review analyzed the functional, psychological, and social/behavioral impacts of unilateral hearing loss on adult life.
The impact of UHL/AHL/SSD arises because of the inability to effectively and appropriately use binaural hearing (interaural timing differences, interaural loudness differences, binaural squelch, binaural summation, and more) because the peripheral auditory system is unable to send an approximately bilaterally symmetric and/or complimentary signal to the brain. Inability to effectively utilize binaural cues typically causes impairment in the ability to identify the origin of sound in space. Specifically, UHL/AHL/SSD often makes it impossible to know where to focus one’s hearing/listening effort (ie, to know where to attend/focus) along the horizontal and vertical axis.
Further, distance estimation requires the central nervous system to perform an almost-instantaneous analysis of the interaural acoustic information. This analysis includes comparing and contrasting interaural loudness differences (ILDs) across the entire audible spectrum, as well as comparing interaural timing differences (ITDs) with respect to phase, recency, and primacy effects. Binaurally gathered auditory information must then be integrated with binaural summation and binaural squelch to determine which sounds to attend to, which sounds to ignore, and to know where the sound came from. This means binaural hearing does not merely make sound louder by 2-3 dB; binaural hearing allows and facilitates a highly sophisticated soundscape analysis which helps us decode and comprehend speech in noise (SIN), facilitates spatial orientation, and helps us determine our attention and focus.
Due to the challenges inherent in loss of binaural hearing function, unilateral hearing loss is associated with multiple negative consequences and outcomes, including but not limited to:
- Speech-in-noise problems
- Localization ability
- Balance problems
- Speech and language delays
- Auditory processing disorders
- General communication difficulties
- Social/emotional delays
- Academic and behavioral difficulties
Therefore, early diagnosis and management is tremendously important (see the article by Anne Marie Tharpe, PhD, in this special edition of Hearing Review for more information.)
Treatments for UHL/AHL/SSD
For adults, the primary treatment for UHL/AHL/SSD remains contralateral routing of signal (CROS) hearing aids. The essential idea of a CROS hearing aid fitting is that a single microphone is located on the poorer ear and the receiver (via wired or wireless routing) is located on the better/normal-hearing ear. In cases where both ears may benefit from amplification, yet one ear is significantly more able to interpret/comprehend sounds, a binaural contralateral routing of signal strategy (BiCROS) is used. In a BiCROS fitting, two microphones are placed (one on each ear), yet the receiver (via wired or wireless routing) is located on the better hearing ear. Therefore, a CROS fitting involves one microphone whereas a BiCROS involves two microphones. In both systems, the total sound is delivered to the better hearing ear.
Other solutions for UHL/AHL/SSD include methods through which sound is delivered to the better hearing ear via bone-conduction stimulation. In the case of a transcranial CROS, very loud hearing aids are placed on the worse ear, such that interaural loudness thresholds are exceeded and the better hearing ear perceives the sound from the worse ear via bone conduction. Surgical treatments such as bone-anchored or osseointegrated solutions take advantage of this bone-conduction strategy as well, and in some situations, cochlear implantation of the poorer ear is a viable option (see the article by Amanda O’Donnell, AuD, and Allison Racey, AuD, in this edition for more information). For the remainder of this article, we will focus on CROS and BiCROS hearing aid fittings.
Evaluation of CROS and BiCROS Success
Clinical use of CROS and BiCROS strategies has resulted in varied outcomes, with some patients and clinicians reporting great success and others reporting insufficient benefit to warrant the treatment. Subjective reports sometimes contrast with the evidence-based literature—which shows that the benefits of traditional CROS and BiCROS fittings have historically been ambiguous.
One reason for this ambiguity is that the concept of “success” has many facets, and different studies tend to measure these outcomes in different ways. A recent consensus document was created to propose a unified testing framework for research involving treatment outcomes for single-sided deafness and asymmetric hearing loss,3 yet a consistent strategy has not been used in contemporary research.
In reviewing the CROS and BiCROS literature, we have arbitrarily limited evidence to the past decade, as newer hearing aid technologies likely allow for better outcomes, and the majority of these products remain commercially available. In 2012, Williams, McArdle, and Chisolm11 found that newer BiCROS technology outperformed older BiCROS technology in a sample of 39 veterans. Interestingly, the data suggested their findings were likely due to the previously fit technologies not providing adequate gain in the better hearing ear.
With regard to acceptance and usage of CROS and BiCROS systems, the data are underwhelming. Leterme and colleagues12 found that only 11% of their patients elected to obtain CROS devices. Purcell et al13 found that 31% of children in their institution rejected CROS devices, citing discomfort and lack of benefit as reasons for non-use. With regard to BiCROS technology, Oeding and Valente14 similarly found that only 33% of the patients in their study elected to retain their BiCROS instruments. On the other hand, Williams, McArdle, and Chisolm11 had 95% of patients who elected to keep their newer BiCROS instruments. However, it should be noted that these were all previous consistent users of BiCROS instruments, many of whom were under-fit with regard to gain, and they were provided instruments at no out-of-pocket cost by the Veterans Administration.
When considering objective outcomes, there are numerous ways to measure benefit. Most commonly, subjects are tested on their ability to localize sound and to understand speech in noise. Regarding localization, it is known that the brain uses interaural timing and intensity differences to locate sound. Because the CROS/BiCROS system strategy transmits sound to only one ear, there is no reason to hypothesize that people using such systems can localize sound. This is borne out in the data, demonstrating time and again CROS/BiCROS systems do not provide listeners with the ability to localize sound.15-19 There may, however, be some benefit as far as lateralization of sound sources (awareness of which side of the listener the sound emanates).16,17
Another common outcome measure for these devices is speech perception in background noise. Here, the evidence is more nuanced. The answer to whether CROS/BiCROS helps to understand speech in background noise depends largely on the testing paradigm. When speech is presented to the microphone/transmitter of the CROS system, with noise elsewhere, the answer is most often a resounding “yes.”15,16,17,19 When speech is presented to the front of the listener, with noise elsewhere, the answer is equivocal.14-18,20 When noise is presented to the microphone/transmitter of the CROS system, with speech elsewhere, the answer is clearly “no.”15,16,18
Subjective patient benefits are also of great importance, and here the results are even more complex. In many studies, patients report subjective benefit from CROS/BiCROS devices11,14-18,20 even when objective benefit is not overwhelming. One reason a patient may experience subjective benefit while not demonstrating high objective benefit is the placebo effect. Very few studies for any hearing instrumentation attempt to manage this variable.
Another possible reason for greater perceived subjective benefit is that hearing occurs in the brain. In real life, people do not utilize their CROS/BiCROS devices under the sorts of conditions measured in the laboratory. It is known that people cannot localize sound with CROS/BiCROS hearing aids when visual and contextual cues are removed. However, if we provide the brain with additional sources of information, the brain may use the fact that “Uncle Bob is sitting on my right side” (ie, information provided by context and vision) to “localize” his voice to the right side, even when this auditory information is being delivered to the left ear. The speech-in-noise tests used in CROS/BiCROS studies do not typically replicate real-world conditions where the patient often experiences complex environments and where context is often provided to support speech understanding.
We have not found any recent studies in the literature which have explored the phenomenon of how we “hear” and perceive with a CROS/BiCROS system under typical acoustic conditions when coupled to multisensory input and context used by the cognitive system to understand what is happening in the environment and what is being said. It is therefore not surprising that patients using these systems in their unique environments may perceive subjective benefits that are incongruent with objective outcomes obtained under controlled conditions.
Unfortunately, the published research seldom describes the (detailed) hearing status of the poorer ear. We commonly refer to a CROS/BiCROS system as a solution for “single-sided deafness,” but in the reviewed literature the research definition only includes pure-tone threshold and speech perception measures for the poorer ear. None of the papers mentioned any evaluation of binaurally aided function to determine whether sound stimulation of the poorer ear could assist in improving outcomes via the improved spatial hearing only possible with a binaural system. The research also fails to provide clarity because it does not address the participation restrictions or “handicap” experienced by the patient with single-sided deafness.
Donald Hayes, PhD, noted in 2006:
“It is not very realistic to expect substantial benefit with a CROS aid in most types of background noise. The resources required for perceiving speech in a diffuse noise background (localization and figure/ground separation) cannot be provided by a device that only aids one ear. Those skills require binaural input…”21
Discussion
In the clinical world, it seems every hearing care professional has at least one patient who “wouldn’t leave their house without their CROS hearing aid!” And often we hear “my patients love their CROS/BiCROS fitting!” Indeed, many patients do love their CROS/BiCROS hearing aids. We are not disputing this fact.
However, our key point in this 2019 literature update is the same as the point made by Hayes21 over a decade ago: we believe many patients mistake hearing (perceiving sound) for listening (comprehending the meaning of sounds). That is, because their CROS/BiCROS hearing aid makes the world a little louder, they believe they are “hearing better”—and absolutely, in some respects, they are. However, as hearing care professionals, we know the most typical goal of a hearing aid fitting is to improve the wearer’s speech-in-noise ability. With regard to that goal, unless the person speaking is doing so very near the microphone of the CROS/BiCROS in a speech babble situation, it is unlikely there is an actual measurable improvement in speech in noise. ?
References
-
Lipschitz N, Kohlberg GD, Scott M, Greinwald JH. Imaging findings in pediatric single-sided deafness and asymmetric hearing loss. Laryngoscope. 2019;May 27. doi: 10.1002/lary.28095. [Epub ahead of print.]
-
Bowers D. Unilateral hearing loss in children: Impact and solutions. May 15, 2017. Available at: https://www.audiologyonline.com/articles/unilateral-hearing-loss-in-children-19953
-
Van de Heyning P, Távora-Vieira D, Mertens G, et al. Towards a unified testing framework for single-sided deafness studies: A consensus paper. Audiol Neurotol. 2017;21:391-398. Available at: https://www.ncbi.nlm.nih.gov/pubmed/28319951
-
Vincent C, Arndt S, Firszt JB, Fraysse B, Kitterick PT, Papsin BC, Snik A, Van de Heyning P, Deguine O, Marx M. Identification and evaluation of cochlear implant candidates with asymmetrical hearing loss. Audiol Neurotol. 2015;20[suppl 1]:87-89.
-
Kuhn M, Heman-Ackah SE, Shaikh JA, Roehm PC. Sudden sensorineural hearing loss: A review of diagnosis, treatment, and prognosis. Trends Amplif. 2011;15(3)[Sept]:91-105. doi: 10.1177/1084713811408349 PMCID: PMC4040829
-
Fal M, Piechocki J, Morawska-Kochman M, et al. Sudden hearing loss treated with hyperbaric oxygen (HBO): Case study. Pol Hyperb Res. 2015;51:7-10.
-
Miller MH. Introduction to special issue: Sudden hearing loss: Unique challenges and opportunities. Hearing Review. 2003;10(13):16-18. Available at: https://hearingreview.com/2003/12/sudden-hearing-loss-unique-challenges-and-opportunities
-
Hear-It.org. Unilateral hearing loss–Single sided deafness. Undated. Available at: www.hear-it-org/single-sided-deafness
-
Meehan S, Hough EA, Crundwell G, Knappett R, Smith M, Baguley DM. The impact of single-sided deafness upon music appreciation. J Am Acad Audiol. 2017 May;28(5):444-462. doi: 10.3766/jaaa.16063.
-
Galloway J, Zhang V, Marnane V, Hou S, Stewart G, Bardy F. The impact of unilateral hearing loss on adult life. Hearing Review. 2019;26(4)[Apr]:10-14. Available at: https://hearingreview.com/2019/03/impact-unilateral-hearing-loss-adult-life/
-
Williams, VA, McArdle, RA, Chisolm, TH (2012). Subjective and objective outcomes from new BiCROS technology in a veteran sample. J Am Acad Audiol. 2012;23:789-806.
-
Leterme G, Bernardeschi D, Bensemman A, Coudert C, Portal JJ, Ferrary E, Sterkers O, Vicaut E, Frachet B, Bozorg Grayeli A. Contralateral routing of signals hearing aid versus transcutaneous bone conduction in single-sided deafness. Audiol Neurotol. 2015;20(4), 251-260.
-
Purcell PL, Jones-Goodrich R, Wisneski M, Edwards TC, Sie KCY. Hearing devices for children with unilateral hearing loss: Patient- and parent-reported perspectives, Int J Ped Otorhinolaryngol. 2016;90:43-48.
-
Oeding K, Valente M. Sentence recognition in noise and perceived benefit of noise reduction on the receiver and transmitter sides of a BICROS hearing aid. J Am Acad Audiol. 2013;24:980-991.
-
Kitterick PT, Nelson Smith S, Lucas L. Hearing instruments for unilateral severe-to-profound sensorineural hearing loss in adults: a systematic review and meta-analysis. Ear Hear. 2016;37(5):495-507.
-
Kuk F, Seper E, Lau C, Crose B, Korhonen P. Effects of training on the use of a manual microphone shutoff on a BiCROS device. J Am Acad Audiol. 2015;26:478-493.
-
Ryu N-G,Moon IJ, Byun H, Jin SH, Park H, Jang K-S, Cho Y-S. Clinical effectiveness of wireless CROS (contralateral routing of offside signals) hearing aids. Eur Arch Otorhinolaryngol. 2015;272:2213-2219.
-
Snapp HA, Holt FD, Liu X, Rajguru SM. Comparison of speech in noise and localization benefits in unilateral hearing loss subjects using contralateral routing of signal hearing aids or bone anchored implants. Otol Neurotol. 2017;38(1):11-18.
-
Snapp HA, Hoffer M, Liu X, Rajguru SM. Effectiveness in rehabilitation of current wireless CROS technology in experienced bone anchored implant users. Otol Neurotol. 2017;38(10):1397-1404.
-
Finbow J, Bance M, Aiken S, Gulliver M, Verge J, Caissie R. A comparison between wireless CROS and bone-anchored hearing devices for single-sided deafness: A pilot study. Otol Neurotol. 2015;36:819-825.
-
Hayes D. A practice guide to CROS/BiCROS fittings. July 24, 2006. Available at: https://www.audiologyonline.com/articles/practical-guide-to-cros-bicros-977

Douglas L. Beck, AuD

Virginia Ramachandran, AuD, PhD
About the authors: Douglas L. Beck, AuD, is Executive Director of Academic Sciences and the guest-editor of this special edition of Hearing Review. Virginia Ramachandran, AuD, PhD, is Education and Training Specialist at Oticon Inc in Somerset, NJ.
Correspondence can be addressed to Dr Beck at: [email protected]
Citation for this article: Beck DL, Ramachandran V. Contralateral routing of signal: A status report 2019. Hearing Review. 2019;26(10):12-16.
About this month’s guest-editor: The Hearing Review thanks Douglas L. Beck, AuD, for guest-editing this month’s special edition (October 2019 HR). Dr Beck earned his master’s degree at the University of Buffalo and his doctorate from the University of Florida, then began his distinguished career at the House Ear Institute in Los Angeles, working in cochlear implant research and intraoperative cranial nerve monitoring. In 1988, he became Director of Audiology at Saint Louis University, and 8 years later co-founded a multi-office dispensing practice in St Louis. From 1999-2005, he served as President and Editor-in-Chief of AudiologyOnline.com, SpeechPathology.com, and HealthyHearing.com, until joining Oticon. While with Oticon, he also served as Web Content Editor for the American Academy of Audiology (AAA) from 2008–2015, and in 2016 became the Senior Editor for Clinical Research for our Inside the Research column, and also served as adjunct Clinical Professor of Communication Disorders & Sciences at the State University of New York at Buffalo. In 2017, Oticon appointed him Executive Director of Academic Sciences. Dr Beck is among the most prolific authors in audiology with 180 published articles and more than 1240 abstracts, interviews, and op-eds written for AudiologyOnline (1999-2005), AAA (2008-2015), and The Hearing Review, addressing a wide variety of audiology and professional topics. — Karl Strom, editor
Other articles in the October 2019 Hearing Review special edition on unilateral hearing loss:
- Introduction to Special Edition: Unilateral Hearing Loss: Underappreciated, Undertreated, By Karl Strom
- Contralateral Routing of Signal: A Status Report 2019, By Douglas L. Beck, AuD, and Virginia Ramachandran, AuD, PhD
- Unilateral Hearing Loss in Children: Current Perspectives, By Anne Marie Tharpe, PhD
- A New Dual-Streaming CROS/BiCROS Solution, By Susanna Løve Callaway, AuD, and Pernille Aaby Gade
- Managing People with Sensorineural and Conductive Unilateral Hearing Loss and Single-Sided Deafness, By Amanda O’Donnell, AuD, and Allison Racey, AuD
Also see:
- The Impact of Unilateral Hearing Loss on Adult Life, By James Galloway, MSc; Vicky Zhang, PhD; Vivienne Marnane; Sanna Hou, MClinAud; Greg Stewart, and Fabrice Bardy, PhD



