
Research | June 2017 Hearing Review
The facts about electromagnetic radiation and wireless hearing aid technology
The integration of wireless technology and hearing aids has fundamentally reshaped the direction of the hearing industry. Today, wireless hearing aid users benefit from smartphone connectivity, while future changes to the Bluetooth® standard will permit nearly universal hearing aid interconnectivity. These future hearing aids will do more than adapt to the user’s environment; rather, they will become part of a mesh of wireless devices that interact with any number of other wireless devices in a given space or across a wireless network.
While many patients and hearing care professionals have welcomed advancing interconnectivity, there may be public concerns as the technology becomes more popular. Health concerns regarding radio frequency (RF) electromagnetic radiation remains a concern among consumers, even in spite of 95% of the US population reporting cell phone ownership.1,2
In this article, we will discuss the current state of wireless hearing aid technologies and how wireless hearing aid systems are being designed to be both effective and safe to use.
Health Concerns
While their enabling wireless technologies are not widely understood by the public, RF radiators like cellphones, devices supporting Bluetooth®, and WiFi routers have become ubiquitous. However, the term “radiation” carries a strong negative connotation, a fact recognized by the World Health Organization (WHO) that motivated the creation of material for public education on the topic.3
There are various forms of electromagnetic radiation that vary along a frequency spectrum (Figure 1); some types of radiation pose health risks, while others are not believed to result in negative health effects. The most potentially hazardous form of these two types is ionizing radiation, which has ultra-high frequency photons capable of removing electrons from exposed atoms. This disruptive subatomic process can lead to undesirable long-term effects in body tissues, including damage made to genetic material (ie, DNA) and cellular mutations like cancer.4-6

Figure 1. The health impacts of electromagnetic radiation differ based upon the frequency. Wireless hearing aid technology is non-ionizing and has only theoretical heating properties.
The second type is non-ionizing radiation, which is comparatively benign. Non-ionizing electromagnetic energy is emitted by all wireless devices during communication and has a thermal or warming effect rather than an ionizing effect. According to the WHO, RF energy may be converted into heat energy as it is being absorbed by body tissue, but it is safe within certain dosage levels.3 Some industrial heaters use RF energy for drying; these are the only applications of RF radiation that have been found to raise body temperature by more than 1° C. The thermal effects of low-powered wireless radiators (ie, consumer electronic devices and hearing aids) are almost non-existent.
The possibility of non-thermal health effects due to non-ionizing radiation are an ongoing topic of discussion within the scientific community. Several case-control studies suggested an increased risk for gliomas tumors due to cellphone use.7-9 However, a large-scale epidemiological study, funded by the National Institutes of Health (NIH) and the National Cancer Institute, countered these results by concluding that the projections were not consistent with documented medical trends. Specifically, if the effects of cellphone use on glioma risk were to have been assumed to be accurate, the incidence rates would be 44% higher than those actually observed within that time frame.10
Numerous organizations and government agencies, who each share an interest in promoting public health, occupational safety, and environmental protection, have helped to shape many of the global wireless safety regulations.11 The WHO and the Federal Communications Commission (FCC) have both stated that, even in the presence of evidence that confirms safety, the organizations will continue to monitor and promote research relating to the possible health impacts that might result from non-ionizing RF radiation.3,11 Clinicians should feel comfortable with the recommendations of these governing authorities and remain cognizant of the body of audiological literature that is overwhelmingly in support of wireless hearing aid and cochlear implant system capabilities when formulating evidence-based treatment decisions for patients.12,13
Wireless Regulations
Wireless technologies, including those used by the hearing aid industry, are strictly regulated to ensure both public safety and communication reliability are maintained. Even governments in developing countries have adopted regulations consistent with those enforced in the United States or the European Union (EU).
In the United States, wireless hearing aids are classified as Class II medical devices while traditional hearing aids are classified as Class I medical devices. This elevated classification requires that wireless hearing aids conform to the regulations set forth by both the US Food and Drug Administration (FDA) and the FCC. Similarly, wireless hearing aids must conform to both the Medical Device Directive14 and Radio Equipment Directive15 in order to become certified for distribution within the EU.
The regulations set forth by the FCC and Radio Equipment Directive each define the appropriate frequency bands and respective broadcast strengths at which wireless devices may communicate. Much like air traffic control, these wireless regulations were established to prevent overcrowding certain frequency bands, which could lead to excessive interferences. Limits on overall power output also serve to protect the population from being exposed to hazardous levels of electromagnetic radiation.
The wireless regulations currently in place were developed with health concerns in the forefront:
“The [FCC] carefully considered the large number of comments submitted in its rule-making proceeding, and particularly those submitted by the U.S. Environmental Protection Agency (EPA), the FDA, and other federal health and safety agencies. The new guidelines…represent a consensus view of the federal agencies responsible for matters relating to public safety and health.”16
In terms of public safety, Specific Absorption Rates (SAR) are, perhaps, even more informative than output energy levels. In fact, the FCC states that “Guidelines for human exposure to RF fields are based on SAR thresholds where adverse biological effects may occur.”16 Theoretically, RF radiation could become problematic when an excessive amount of energy is absorbed by body tissues. Similar to how excessive exposure to the sun’s ultraviolet (UV) radiation causes sunburn and could eventually lead to increased risk of melanoma,17 high levels of absorbed RF energy could cause body tissue to heat up and potentially cause damage to the living cells within the body.
At extreme levels, non-ionizing electromagnetic radiation would act similarly to how food is heated within a microwave oven. Therefore, the FCC and the Radio Equipment Directive each regulate the maximal SAR levels at which wireless devices may operate. The regulations which regulate wireless hearing aid Output Power and SAR are summarized for the US and EU in Table 1.
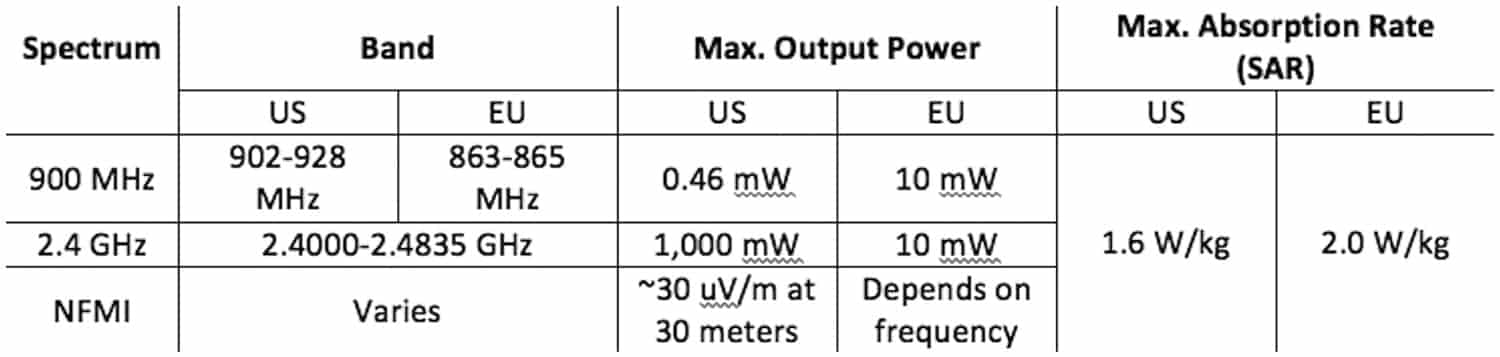
Table 1. Summary of maximum allowable output and Specific Absorption Rate (SAR) limits which govern wireless hearing aids in the United States18,19 and the European Union.20-23 The Output Power data were converted from dBm to mW for comparison.
By design, hearing aids radiate extremely low levels of energy; therefore, the levels of electromagnetic energy that wireless hearing aids radiate are well below the maximum levels permitted by governing regulations. The amount of conducted power output for various 2.4 GHz hearing aids are compared to the conducted power output of a representative smartphone in Figure 2. Based on these measured data, it is reasonable to conclude that the conducted power of 2.4 GHz hearing aids are significantly lower than those of cellular phones.
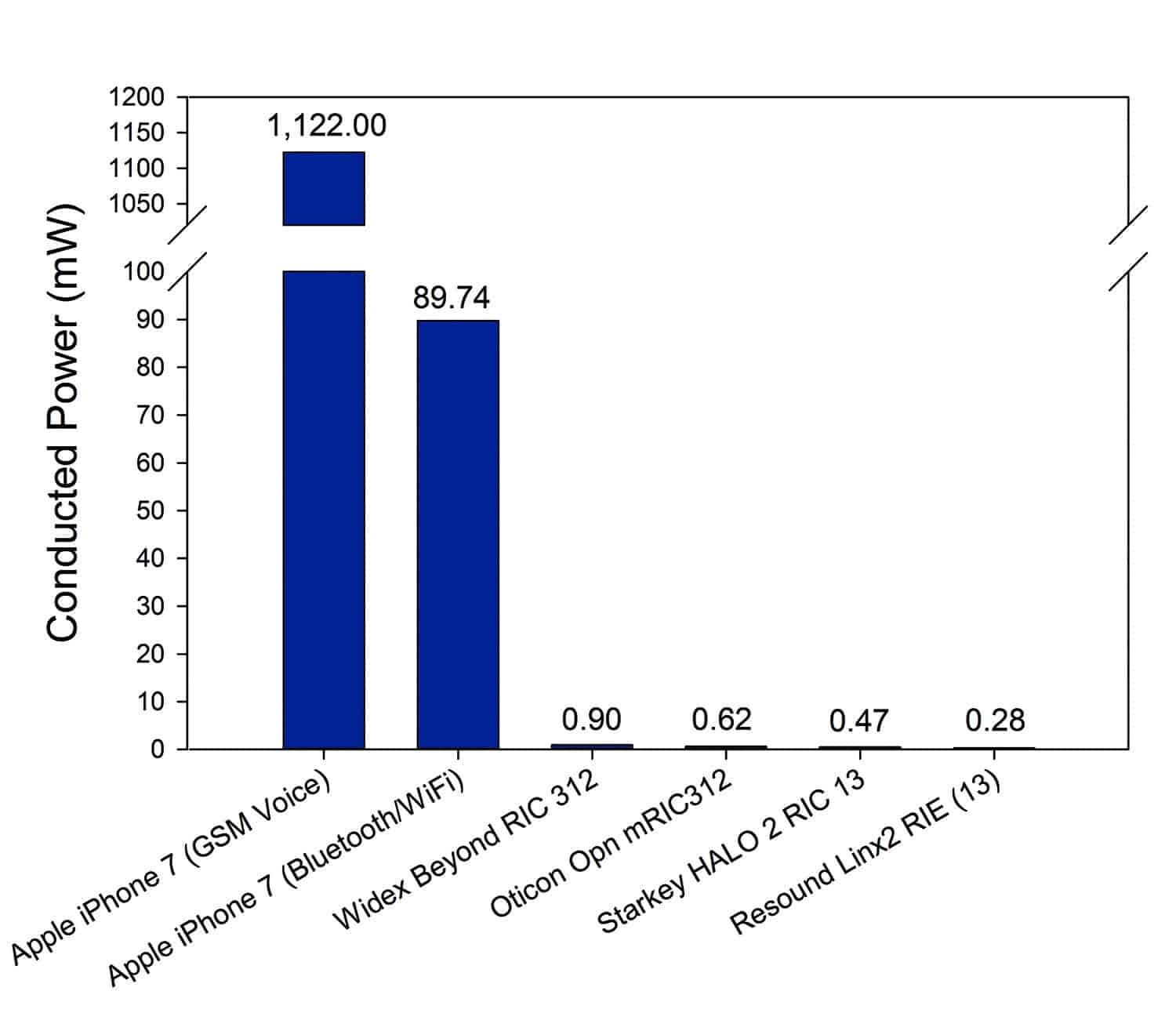
Figure 2. Summary of the conducted RF power output measurement of the Apple® iPhone® 7 (model A1660)24,25 and various 2.4 GHz wireless hearing aids are plotted.26-29 The GSM Voice measurement was made at 1900 MHz.
The typical SAR values for wireless hearing aids range between 0.001-0.02 W/kg. In other words, the amount of electromagnetic radiation absorbed from wireless hearing aids is anywhere between 80 to 2,000 times less than what regulations would allow (1.6-2.0 W/kg). The variability in this range is directly tied to the wireless technology and radio frequency spectrum used in the device. At these measured levels, a patient would have to wear either 75 individual hearing aids that broadcast at 2.4 GHz or 1,125 individual hearing aids that broadcast at 900 MHz, simultaneously, in order to absorb the same amount of energy that we experience when holding a mobile phone to our ear.
Prior to being released to the market, a wireless hearing aid’s conformity to each country’s wireless regulations is certified. In the United States, a third-party Telecommunications Certification Body (TCB) laboratory must measure and certify the device’s compliance to FCC standards.29 A TCB is then also able to audit the manufacturer’s devices’ for ongoing conformance, at any time, following the certification of the device. It should also be noted that each wireless hearing aid must meet the wireless standards of the country in which they are intended to be used, not the regulations of the device’s country of origin.
Wireless Hearing Aid Design
Hearing aid manufacturers strive to optimize their wireless hearing aid offerings both in terms of connection reliability as well as power efficiency. Variance across patients and listening conditions can make optimizing wireless hearing aid systems a complex process.
Factors such as connection distance, proximity of reflective surfaces, interference from other wireless devices, and energy loss through body absorption must all be factored into the hearing aid design. For example, indoor wireless performance may be very different from wireless performance experienced outdoors, where the only reflective surface may be the ground on which the hearing aid user is standing. Furthermore, individual differences in body geometry increase the variability that wireless engineers must account for when designing a system that provides each user with a consistent and reliable experience.
The RF radiation of hearing aids is so slight that highly specialized equipment must be used to measure and optimize the performance of hearing aid prototypes. At Starkey Hearing Technologies, wireless engineers leverage a state-of-art, anechoic SATIMO chamber (Figure 3) to measure the propagation of RF radiation from various antennae and hearing aid designs. Simulations and measurements can be performed either in free space, fixed to a mannequin head, or worn by a research participant. The goal of wireless optimization is to provide consistent signal transmission and reception while using the least amount of energy possible. An emphasis on energy efficiency maximizes battery life and allows for more signal processing resources.

Figure 3. Mannequin head placed within the anechoic SATIMO chamber at Starkey Hearing Technologies’ research facility in Eden Prairie, Minn.
Summary
As awareness of wireless hearing technology grows, hearing healthcare professionals may notice an uptick in long-term safety concerns. Consumers should be confident knowing that wireless hearing aids are safe and strictly regulated medical devices that meet governmental wireless communication standards in addition to those set forth for medical devices.
References
-
Arning K, Kowalewski S, Ziefle M. Health concerns versus mobile data needs: Conjoint measurement of preferences for mobile communication network scenarios. Human and Ecological Risk Assessment: An International Journal. 2014;20(5):1359–1384. Available at: https://doi.org/10.1080/10807039.2013.838127
-
Pew Research Center. Mobile Fact Sheet. January 12, 2017. Available at: http://www.pewinternet.org/fact-sheet/mobile
-
World Health Organization (WHO). Electromagnetic fields and public health. May 2006. Available at: http://www.who.int/peh-emf/publications/facts/fs304/en
-
US Nuclear Regulatory Commission. NRC: Glossary–Ionizing radiation. April 10, 2017. Available at: https://www.nrc.gov/reading-rm/basic-ref/glossary/ionizing-radiation.html
-
US Environmental Protection Agency (EPA). Radiation basics. May 18, 2017. Available at: https://www.epa.gov/radiation/radiation-basics
-
US Environmental Protection Agency (EPA). Radiation health effects. May 18, 2017. Available at: https://www.epa.gov/radiation/radiation-health-effects
-
Oster E. Cellphones do not give you brain cancer. January 6, 2015. Available at: https://fivethirtyeight.com/features/cellphones-do-not-give-you-brain-cancer
-
Hardell L, Carlberg M. Mobile phone and cordless phone use and the risk for glioma – Analysis of pooled case-control studies in Sweden, 1997–2003 and 2007–2009. Pathophysiol. 2015;22(1):1-13. Available at: https://doi.org/10.1016/j.pathophys.2014.10.001
-
INTERPHONE Study Group. Brain tumour risk in relation to mobile telephone use: results of the INTERPHONE international case-control study. International J Epidemiol. 2010;39(3):675–694. Available at: https://doi.org/10.1093/ije/dyq079
-
Little MP, Rajaraman P, Curtis RE, et al. Mobile phone use and glioma risk: comparison of epidemiological study results with incidence trends in the United States. Brit Med J. 2012;344(March 08, 1):e1147–e1147. Available at: https://doi.org/10.1136/bmj.e1147
-
US Federal Communications Commission (FCC). Wireless devices and health concerns. November 1, 2016. Available at: https://www.fcc.gov/cgb/consumerfacts/mobilephone.pdf
-
Rodemerk KS, Galster JA. The benefit of remote microphones using four wireless protocols. J Am Acad Audiol. 2015;26(8):724-731. Available at: https://doi.org/10.3766/jaaa.15008
-
Wolfe J, Morais Duke M, Schafer E, Cire G, Menapace C, O’Neill L. Evaluation of a wireless audio streaming accessory to improve mobile telephone performance of cochlear implant users. Intl J Audiol. 2016;55(2), 75-82. Available at: https://doi.org/10.3109/14992027.2015.1095359
-
The European Parliament and of the Council of the European Union. Directive 2007/47/EC of the European Parliament and of the Council of 5 September 2007 amending Council Directive 90/385/EEC on the approximation of the laws of the Member States relating to active implantable medical devices, Council Directive 93/42/EEC concerning medical devices and Directive 98/8/EC concerning the placing of biocidal products on the market. September 5, 2007. Available at: http://ec.europa.eu/consumers/sectors/medical-devices/files/revision_docs/2007-47-en_en.pdf
-
The European Parliament and of the Council of the European Union. Directive 2014/53/EU of the European Parliament and of the Council of 16 April 2014 on the harmonisation of the laws of the Member States relating to the making available on the market of radio equipment and repealing Directive 1999/5/EC. September 5, 2007. Available at: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32014L0053&from=EN
-
US Federal Communications Commission Office of Engineering & Technology. OET Bulletin 65. 1997. Available at: https://transition.fcc.gov/Bureaus/Engineering_Technology/Documents/bulletins/oet65/oet65.pdf
-
Newton-Bishop JA, Chang YM, Elliott F, et al. Relationship between sun exposure and melanoma risk for tumours in different body sites in a large case-control study in a temperate climate. Euro J Cancer. 2011;47(5):732-741. Available at: https://doi.org/10.1016/j.ejca.2010.10.008
-
US Federal Communications Commission. Code of Federal Regulations, 47 C.F.R. § 15, (2015). Available at: https://www.fcc.gov/general/rules-regulations-title-47
-
US Federal Communications Commission. Code of Federal Regulations, 47 C.F.R. § 2.1093, (2010). Available at: https://www.gpo.gov/fdsys/granule/CFR-2010-title47-vol1/CFR-2010-title47-vol1-sec2-1093
-
ETSI EN 300 328 v 2.1.1, Electromagnetic compatibility and Radio spectrum Matters (ERM); Wideband transmission systems; Data transmission equipment operating in the 2.4 GHz ISM band and using wide band modulation techniques; Harmonized EN covering the essential requirements of article 3.2 of Directive 2014/53/EU, 2016.
-
ETSI EN 300 330-1 V1.8.1 2.1.1, Short Range Devices (SRD); Radio equipment in the frequency range 9 kHz to 25 MHz and inductive loop systems in the frequency range 9 kHz to 30 MHz; Harmonised Standard covering the essential requirements of article 3.2 of Directive 20152014/53/EU, 2017.
-
ETSI EN 300 422-1 V1.5.1, Electromagnetic compatibility and Radio spectrum Matters (ERM); Wireless microphones in the 25 MHz to 3 GHz frequency range; Part 1: Technical characteristics and methods of measurement. June 2015.
-
1999/519/EC: Council Recommendation of 12 July 1999 on the limitation of exposure of the general public to electromagnetic fields (0 Hz to 300 GHz). Official Journal of the European Union. 1999;42(L199/59):59-70.
-
UL Verification Services Inc. Certification Test Report for Cellular Phone with Bluetooth and WLAN Radios Model Number: A1660, A1780 (No. 16U23309-E6V4). Fremont, Calif: UL;2016. Retrieved from FCC Equipment Authorization Database.
-
UL Verification Services Inc. Certification Test Report for Cellular Phone with Bluetooth and WLAN Radios Model Number: A1660, A1780 (No. 16U23309-E1V4). Fremont, Calif: UL;2016. Retrieved from FCC Equipment Authorization Database.
-
AT4 Wireless. Test Report for Wireless hearing instrument Model: BRIE (No. 43932RRF.002). Málaga, España. 2014. Retrieved from FCC Equipment Authorization Database.
-
CETCOM ICT Services. Test Report for Wireless hearing instrument Model: Aurora mini RITE (No. 1- 0682/15-2–7). Saarbruecken, Germany. 2015. Retrieved from FCC Equipment Authorization Database.
-
Element Materials Technology Warwick Ltd. Report on the Radio Testing For Widex A/S on Widex Beyond Fusion2 (Model. B-F2) (No. TRA-029062-01-45-04B). London, England. 2016. Retrieved from FCC Equipment Authorization Database.
-
US Federal Communications Commission. Code of Federal Regulations, 47 C.F.R. Part 2, Subpart J-Equipment Authorization Procedures (2015).
CORRESPONDENCE can be addressed to HR or Dr Burwinkel at: [email protected]
About the Authors
Justin R. Burwinkel, AuD, is a Research Audiologist; William J. Mitchell, MSEE, is a Wireless Regulatory Engineer; Ezdeen Elghannai, PhD, is a Senior Radio Design Engineer, and Jason A. Galster, PhD, is Manager of Audiology Research for Starkey Hearing Technologies in Eden Prairie, Minn.
Citation for this article. Burwinkel JR, Mitchell WJ, Elghannai E, Galster JA. Do Wireless Hearing Aids Present a Health Risk? Hearing Review. 2017;24(6):34-40.


One thing that has not apparently been addressed in the paper or discussion is exposure time. I’m comfortable using my Bluetooth mouse or cellphone from time to time, but the hearing aid needs to be in intimate contact with my head for prolonged periods every day. As the aids communicate with each other, the signals go straight through my brain. I know that manufacturers claim that signals propagate around the head, but given that radio waves naturally travel in straight lines, this argument is not very convincing.
A related point for me is distance. Radio signals decay at one over distance squared, so as long as my head is more than a couple of feet away from a source such as a modem, I’m not too worried. But wireless hearing aids don’t allow me that possibility of distance.
While I’m not an expert on the subject, the FDA has established safety standards for wearable medical devices that use wireless technology (Class 2 devices), and these include hearing aids along with other medical devices, many of which are implantable or in constant contact with the body. I think the article demonstrates pretty clearly that the energy emitted by wireless hearing aids is a fraction of what can be found in most devices–and tiny in comparison to the cell phones most of use carry around in our pockets or purses. It would seem to me (and this is the point of the FDA’s source material, too) that if there were long-term metabolic health effects from these devices, we’d be seeing them by now after all this time. To your point, a wide swath of the population (including me) has their hands on a mouse and keyboard and head 1-2 ft from a monitor for 6-8 hours a day for the past 2-3 decades. There may be a lot of OTHER negative effects, but metabolic changes in our bodies due to RF’s don’t appear to be one of them.
My doctor told me that I was susceptible to EMF’s and pesticides. Having a history of Non-Hodgkins Lymphoma beginning in 1995 in the 4th and last stage, I am concerned about using the new hearing aids even though my hearing requires such hearing aids.I was wondering if I were to use the blue-tooth compatible hearing aids and turned that part off and just used the device working from the batteries, would that emit fewer EMF’s while still enabling my hearing?
There’s a more important question than
“does your hearing device COMPLY with Govt Regulations?
and that is
“does your hearing aid in fact produce the actual radiation that is CAUSING your new-felt headaches?”
There is research evidence indicating damage to the auditory system from use of wireless phones. There is also research evidence that even small amounts of RF such as from hearing aids can impact the brain.
Medeiros, Luisa Nascimento and Tanit Ganz. “Tinnitus and cell phones: the role of electromagnetic radio frequency radiation.” Brazilian Journal of Otorhinolaryngology, vol. 82, no. 1 2015, 97-104.
EMRFR can penetrate exposed tissues and safety exposure levels have been established. These waves provoke proved thermogenic effects and potential biological and genotoxic effects. Some individuals are more sensitive to electromagnetic exposure (electrosensitivity), and thus, present earlier symptoms. There may be a common pathophysiology between this electrosensitivity and tinnitus.
Conclusion: There is already reasonable evidence to suggest caution for using mobile phones to prevent auditory damage and the onset or worsening of tinnitus.
Özgür A, et al. “Effects of chronic exposure to electromagnetic waves on the auditory system.” Acta Otolaryngol, vol. 135, no. 8, 2015, pp. 765-70.
The results support that chronic electromagnetic field exposure may cause damage by leading to neuronal degeneration of the auditory system.
Seckin E, et al. “The effect of radiofrequency radiation generated by a Global System for Mobile Communications source on cochlear development in a rat model.” Journal of Laryngology and Otology, vol. 128, no. 5, 2014, pp. 400-5.
Electron microscopic evaluation revealed significant differences among the groups with regard to the number of normal, apoptotic and necrotic cells. Conclusion: The findings indicated cellular structural damage in the cochlea caused by radiofrequency radiation exposure during cochlear development in the rat model.
There is a list of research on this at https://ehtrust.org/science/research-on-wireless-health-effects/
I think there IS current debate about CELL PHONE radiation and its possible impact on human tissues, although the data seems to tilt heavily on the safe side for cell phones. The FDA believes there is little evidence for RF radiation from cell phones being a health risk when the devices comply with their standards, and the American Cancer Society has no official position on the electromagnetic safety of cell phones (they have a great website page on cell phones and radiation risk). However, what is at issue here is the safety or risk factors associated with WIRELESS HEARING AID use and RF radiation. As this article points out, “At these measured levels, a patient would have to wear either 75 individual hearing aids that broadcast at 2.4 GHz or 1,125 individual hearing aids that broadcast at 900 MHz, simultaneously, in order to absorb the same amount of energy that we experience when holding a mobile phone to our ear.” My point: it’s possible to debate whether cell phones pose a health risk, because there are some studies in peer-reviewed scientific journals that give one pause; however, it would seem highly unlikely–due to the 1 Volt battery and power levels attainable in hearing aids (and now Bluetooth Low-Energy Audio)–that these same studies would apply to the actual radiation coming from a wireless hearing aid. Unless you decide and somehow figure out how to wear 75 wireless hearing aids on your head simultaneously, as this study points out.
To be more accurate, the ionic composition of cochlear fluids is negatively affected by the presence of dissimilar ionization products stemming from wireless connectivity. I think that the neurotransmitter triggers are affected, and sustained use of connectivity may permanently impair neuro-stimulation within the cochlea. This may account for the 10-12db changes in the higher frequencies after the use of connectivity for a year or more!
Good day,
Interesting.
I have been trying new Phonak wireless aides for a month.
Usually, I can get by, free of aides, in the morning with my family. Today, I was unable to hear them at all.
Thus my research.
Thank you.