The occlusion effect (OE) is the sensation of increased loudness (measured also as an increase in sound pressure level)—especially in the low frequencies—that a person experiences to self-generated sounds (vocalization, chewing, swallowing, walking, etc). The problem often occurs when the ears are covered or the ear canal is obstructed (occluded).
The OE is reported generally as an unpleasant sound quality sensation (hollow, boomy, or muffled). It is a consequence of a signal generated peripheral to the tympanic cavity (Figure 1), with the transmission of some of this increased SPL through the normal air-conduction pathway.1 The OE is a long-standing, continuing problem with hearing aid fittings, the resolution of which is considered necessary for successful hearing aid use.
The OE has been documented from bone-conduction measurements made by occluding the ears.1-16 These authors reported the increase in loudness as improvement of bone-conduction thresholds, especially in the low frequencies (250 Hz), by as much as 30 dB (Figure 2), depending on the type of earphone used to occlude the ears.
OE was subsequently reported for hearing aid earmolds acting as occluding devices.17-19 In spite of these observations, the real significance of the OE on hearing aid wearer problems was not truly appreciated until its magnitude (13-25 dB) was measured to self-generated speech using standard (ie, terminating in the outer 1/3, or cartilaginous portion, of the ear canal) earmold/earpiece insertion depths.20-22 Killion et al.21 demonstrated that the magnitude of the occlusion effect varied, with a deeper and full-contact fit in the bony portion of the ear canal providing the least occlusion effect.
Two acoustic approaches have proven successful in managing the OE for hearing aid wearers: larger vents or deeply fitted instruments. The use of vents of 2 mm or greater in diameter within an earpiece (ie, a fairly open earmold fitting) has been studied by several researchers.20,22-25 A difficulty with such fittings is that, when the vent is large and the patient requires more gain, the approach often leads to acoustic feedback, ringing, near-oscillation, or undesirable transient distortion. And, although acoustic feedback can be controlled by the use of notch filters or the rolling off of high frequencies, these approaches result in the loss of significant high-frequency information considered necessary for many patients to understand speech.
The second method is to reduce or eliminate the occlusion effect using deeply fitted hearing aids or earmolds (with no vents) that make full contact with the bony structure of the ear canal.26-30 Deeply fitted hearing aids can be problematic because of discomfort, difficulty with correct ear impressions, lack of knowledge/acceptance of deep-fit acoustic advantages, and lack of “programmed fit” formulae based on deep-fit transfer functions.
Assessing OE with New Device
Hearing device. The PAC (Post Auricular Canal from SeboTek Hearing Instruments) is a new style device that utilizes a linkage from a miniature sound processor to a receiver encapsulated inside selected stock soft tips of varying diameters. The natural placement of the hearing aid receiver deep in the ear canal has been shown to essentially eliminate the occlusion effect with this style instrument.31,32
Although measurements had been reported on the occlusion effect reduction with this system,31 nothing exists to show the consistency of response within or between subjects, or between different test sites. The purposes of this study were to 1) measure the occlusion effect with the PAC; 2) establish consistency of the results within and between subjects with the recommended real-ear measurement procedure, and 3) determine the consistency across test sites.
Subjects. Three different research teams in three different locations (University of Northern Colorado [L1]; University of Oklahoma Health Sciences Center [L2], and a private facility in St. George, Utah [L3]) evaluated 36 adult subjects. Additionally, results from a previous study (Etymotic Research, Elk Grove Village, Ill [L4]) were included for comparison purposes. Ear canals were to be free from cerumen as determined from a visual inspection of the ear canal.
Test Equipment. The PAC (Figure 3) is a device with a separate sound processor and speaker assembly. The speaker was encased in appropriately sized soft and flexible silicone fitting tips and placed deep in the ear canal. Tip sizes were determined for each subject by a sizing tool.
A specific probe-mic measurement procedure that takes advantage of the speaker/tip module was recommended for this study in order to provide a consistent method for making the measurement. As illustrated in Figure 4, a custom-molded hearing aid wax tool is pushed through the tip, the probe is threaded through the loop of the wax removal tool, and the probe is pulled through the tip and adjusted to the proper length. It is important that this process be enacted after the tip has been placed onto the speaker. If not, there is a high probability that the expansion resulting from the speaker being placed in the tip will compress the probe tube, rendering measurements meaningless.
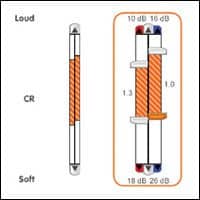
The occlusion effect was measured with the ER-33 Occlusion Effect meter (Figure 5) using a probe tube extending 2 mm beyond the receiver tip. The ER-33 is a hand-held device that measures both the magnitude of the occlusion effect and the leakage around an earmold. For this study, only the occlusion effect data was used.
The subject vocalized the phoneme [i] to produce the occlusion effect. Two microphones of the ER-33 separately measured sound levels outside and inside the ear canal. A digital signal processor calculated the sound levels present at the two microphones and displayed the difference (in dB SPL). The difference in decibels between the sound inside the ear canal and outside the ear represented the amount of occlusion effect. Measurements were made in 2.5 dB increments. The smaller the dB difference, the less the occlusion effect. The meter read accurately over an input range of 60-95 dB SPL, which eliminated the need for a sound level meter to monitor subjects’ vocal efforts.
Procedures. Ten measurements per subject were recorded while the subject produced the phoneme [i]. All testing was done with the PAC sound processor connected, but turned off. The reason for this was to eliminate the gain of the hearing aid as a confusing factor in the measurement of the occlusion effect.
Results
Deep-canal OE measurements were recorded and the results plotted relative to a calculated occlusion effect average of +20 dB for contemporary earpiece fit depths.20-22 Figure 6 shows that the occlusion effect for the three study locations averaged -5.4 dB, with a range from -2.7 dB to -7.4 dB. If an average (estimated from previous studies on the occlusion effect using shallow-fit ear pieces) of +20 dB is used, the deep fit of the test device reduced the magnitude of the occlusion effect 25.4 dB. Although the study from Location 4 (L4) was conducted under somewhat different conditions, the occlusion effect measurement (-3.6 dB) and the standard deviation (4.8) was consistent with those from locations L1, L2, and L3.
Figure 7 plots the 10 repeat measurements for each subject (identified as “series”) from the three test sites. Although the measured occlusion effect differed between test subjects, in all cases the repeated measures by subject were consistent with small intrasubject variability (SD: 0-2.4). Intersubject variability, as expected, was larger but still showed a mean standard deviation between the sites of 4.7 dB (range: 3.7 to 6.3 dB). Not surprising, variances differed between results from the three test sites, but ANOVA and Kruskal-Wallis tests showed no statistical difference between results from the sites at the 0.05 confidence level.
Collectively, the data show that the PAC, with its unique fitting style, substantially reduces or eliminates the occlusion effect. Repeat measurements within and between test subjects show very small variability, as do measurements between test facilities where testing was performed by different clinicians. This indicates that the measurement procedure proposed in this study can be used clinically with accurate and repeatable results when performing similar testing.
Reducing the OE
It is possible that the occlusion effect reduction could be even greater than reported; the lowest measurement allowed by the ER-33 Occlusion Effect Meter is -10 dB, a level reached by a number of subjects. Regardless, the results show that the PAC provides significant reduction of the OE.
It might be argued that 10 successive measurements to an uttered phoneme would not show potential changes in the magnitude of the OE since there was little mandibular movement or time lapse between recordings of the test samples. Figure 8 addresses this question, with the caveat that the measurements are made from a single test subject.33 For this subject, 749 OE measurements were made using five exaggerated mandibular movements between each OE measurement. Additionally, measurements of the OE were made on the same subject using each tip size (sizes 7, 8, 9, 10, 11, 12, and 13 [the tip size corresponds to its diameter in millimeters]), even though a 9-mm tip was the recommended size for this subject. The graph averages show that, regardless of tip size and even with exaggerated mandibular movement between each OE measurement, the speaker assembly remained in position and provided a consistent occlusion effect reading. For this subject, tip sizes 8, 9, and 10 provided similar results, suggesting that a tip size of ±1 mm from the recommended size would provide an appropriate fit. This would seem to hold true for the seal also where measurements were made, even though this was not a part of this study. The crossover of measurements at the 11-mm tip size and continuing to the 12-mm tip size show the continuing impact of a poor seal and increasing OE. Beyond the 12-mm tip size the interaction of the two microphones of the ER-33 Occlusion Effect Meter no longer function properly because the fit is so poor that the sound-level meter readings both attempt to approximate 0 dB since a difference no longer exists between what is measured peripheral and distal to the occluding device.
Placement of the mic probe through the fitting tip (see Figure 4) proved to be very effective in making deep-canal real-ear measurements. This procedure can be used clinically for real-ear probe-mic measurements, as well. A cursory evaluation using round probe-mic tubes and the Frye Electronics Fonix 7000 hearing aid test system allowed for consistent and easy-to-obtain real-ear probe-mic measurements. Following such a measurement, the tip need not be replaced because the opening for the probe mic closes nicely and the tip maintains the seal for hearing aid use. It might be better, however, to use a round object (eg, an appropriately sized needle) to pull the probe through the tip rather than the wax loop used in the illustration.
For this study, the probe used was a crescent-shaped tube recommended for the ER-33 Occlusion Effect Meter. However, the probe was placed through the tip rather than lying alongside the earpiece as recommended. Based on leakage measurements made, this variation did not create any problems with the seal of the earpiece used, and allowed the tube to be positioned properly much more easily.
One should note that the collected data represented here were all obtained on a hearing aid that was not turned on because the interest was in the occlusion effect. Hence, potential acoustical changes related to phase and other uncertainties in a normal use condition are not represented.
An issue that should be mentioned whenever any soft earpiece is placed deeply in the ear canal relates to the temperature of the device when initially inserted (ie, prior to the period when the earpiece becomes warm). The earpiece temperature is generally at or close to unity with the ambient air temperature, but in a short time warms to the patient’s body heat (98.6° F). This additional warmth often allows the earpiece to fit better, especially following mandibular movement, resulting in an improved seal and comfort. This suggests that a short time period might be recommended prior to making certain measurements in the ear canal, such as that for the occlusion effect and for the seal.
Summary
This study measured the magnitude and consistency of the occlusion effect (OE) for a new style of deep-fitting hearing aid, the SeboTek PAC. One of the purported advantages of these instruments is substantial reduction of the OE. Intersubject, intrasubject, and different test-site variability of the occlusion effect was measured on 36 adult subjects. Results indicate that this style of hearing aid fitting reduced the occlusion effect compared to traditional fittings that terminate in the outer 1/3 of the ear canal. The average occlusion effect score was -5.4 compared to an average occlusion effect for traditional fit earmolds of +20 dB,20-22 or an OE improvement of approximately 25 dB.
This fitting approach provides for consistency of OE results within and between subjects. Within-subject variability was excellent (SD: 0-2.4 dB). Inter-subject variability ranged more widely, but the direction and magnitude of the OE reductions were consistent, showing essentially an elimination of the OE with the device.
It was hypothesized that the unique fitting approach of the PAC, coupled with the probe-mic management procedure detailed in this article, would provide consistent OE measurements among the test sites. Indeed, no statistical differences were found. It appears that OE measurements using the technique described with this or similar hearing devices can be compared between test locations and using different examiners.
Acknowledgment
This work was supported by SeboTek Hearing Systems.
| This article was submitted to HR by Wayne J. Staab; PhD, J. Michael Dennis, PhD; H. Christopher Schweitzer, PhD; and Jennifer E. Weber, AuD. Staab is owner of Dr. Wayne J. Staab & Associates, Dammeron Valley, Utah, serves as adjunct professor to Arizona State Univ and the Arizona School of Health Sciences, and is a consultant for Sebotek Hearing Systems LLC, Tulsa, Okla; Dennis is a professor in the Dept of Otorhinolaryngology at the Univ of Oklahoma Health Sciences Center, Oklahoma City, Okla; Schweitzer is president of Hear 4-U International, Lafayette, Colo, and an adjunct professor at the Univ of Northern Colorado, Greeley, Colo; and Weber is assistant professor at the Univ of Northern Colorado. Correspondence can be addressed to Wayne J. Staab, PhD, Wayne J. Staab & Associates, 352 Sundial Ridge Circle, Dammeron Valley, UT 84783; email: [email protected] |
References
1. Feldman AS, Grimes CT, Shur IB. Further studies of the occlusion effect [Technical Report No. 10]. Syracuse, NY: State University of New York; April 1972.
2. Wheatstone C. Experiments on audition. Quarterly J Science Literature Art. 1827;24:67-72.
3. Pohlman A, Kranz F. The problem of middle ear mechanics. Binaural acuity for air and bone transmitted sound under varying conditions in the external auditory canal. Ann Otol Rhinol Laryngol. 1925;34:1224-1238.
4. Pohlman AG. Correlations between the acuity for hearing and bone transmitted sounds in Rinne negative and Rinne positive cases. Ann Otol Rhinol Laryngol. 1930;39:927-960.
5. Kelly N, Reger S. Effect of binaural occlusion of the external auditory meati on the sensitivity of the normal ear for bone conducted sound. J Experim Psychol. 1937;21:211-217.
6. Watson N, Gales R. Bone conduction threshold measurements: effects of occlusion, enclosures and masking devices. J Acoust Soc Am. 1943;18:401-408.
7. Sullivan J, Gotlieb C, Hodges W. Shift of bone conduction threshold on occlusion of the external ear canal. Laryngoscope. 1947;57:690-703.
8. Onchi Y. The blocked bone conduction test for differential diagnosis. Ann Otol Rhinol Laryngol. 1954;63:81-96.
9. Rytzner C. Sound transmission in clinical otosclerosis. Acta Otolaryngol. 1954; [Suppl] 117:1-137.
10. von Békésy G. Experiments in Hearing. New York: McGraw-Hill; 1960.
11. Keyes J, Milburn B. The sensorineural acuity level SAL technique. Arch Otolaryngol. 1961;73:710-716.
12. Studebaker GA. On masking in bone conduction testing. J Sp Hear Res. 1962;5:215-227.
13. Naunton RF. Clinical bone-conduction audiometry. AMA Arch Otolaryngol. 1957;66:281-298.
14. Goldstein DP, Hayes CS. The occlusion effect in bone conduction hearing. J Sp Hear Res. 1965;8:137-148.
15. Dirks D, Swindeman JG. The variability of occluded and unoccluded bone conduction thresholds. J Sp Hear Res. 1967;10, 232-249.
16. Hodgson WR, Tillman TW. Reliability of bone conduction occlusion effects in normals. J Auditory Res. 1966;6:141-151.
17. Huizing EH. Bone conduction: the influence of the middle ear. Acta Otolaryngol. 1960; [Supp].
18. Tyszka F, Goldstein D. Occlusion effect: unilateral sensori-neural hearing loss. J Acoust Soc Am. 1968;43:324-327.
19. Berry RC, Tokay FH. The effect of several occluding devices on BC thresholds and SPLs in the occluded meatus. J Audit Res. 1971;11:1, 69-72.
20. Wimmer VH. The occlusion effect from earmolds. Hearing Instrum. 1986;37:12,19,57-58.
21. Killion MC, Wilber LA, Gudmundsen G. Zwislocki was right…a potential solution to the “hollow voice” problem the amplified occlusion effect with deeply sealed earmolds. Hear Instrum. 1988;39:14-18.
22. Revit LJ. Two techniques for dealing with the occlusion effect. Hear Instrum. 1992;43:12-18.
23. Lybarger SF. Earmold venting as an acoustical control factor. Presentation of Acoustical Factors Affecting Hearing Aid Measurement and Performance. New York: Graduate School of the City University of New York; June 1978.
24. Wynne MK, Williams CN. Can we prevent the sing without plugging up everything? Paper presented at: American Auditory Society Meeting; March 2001, Scottsdale, Ariz.
25. Kiessling J, Margolf-Hackl S, Geller S, Øsergaard O. Researchers report on a field test of a non-occluding hearing instrument. Hear Jour. 2003;56:9, 36-41.
26. Zwislocki J. Acoustic attenuation between the ears. J Acoust Soc Am. 1953;25, 752-759.
27. Berger EH. Tips for fitting hearing protectors. Sound Vibration. 1988;Oct: 22-25.
28. Staab W.J. Deep canal hearing aids: a fitting rationale. Paper presented at: American Auditory Society 16th Annual Meeting; September 1989, New Orleans.
29. Staab WJ, Finlay B. A fitting rationale for deep canal hearing instruments. Hear Instrum. 1991;42:1,6-10,48.
30. Mueller GH. CIC hearing aids: What is their impact on the occlusion effect? Hear Jour. 1994;47:11, 29.
31. Staab WJ. Solving the occlusion effect. Hearing Review. 2004;10:9,46-48, 63.
32. Staab WJ, Schweitzer HC, Dennis JM, Weber J. Occlusion effect results in a deep fitting hearing aid. Paper presented at: American Auditory Society Scientific and Technical Meeting; March 2004, Scottsdale, Ariz.
33. Staab WJ. The hearing aid occlusion effect: past and present: three perspectives. Paper presented at: American Academy of Audiology Annual Convention; April 2004, Salt Lake City, Utah.