By Douglas L. Beck, AuD, and Michael Nilsson, PhD
The literature suggests the number-one complaint of hearing-impaired people and people who wear hearing aids is their inability to clearly understand speech in challenging acoustic environments.1,2 As such, it appears judicious and reasonable to design and incorporate a simple-to-administer, statistically meaningful, and real-life “speech-in-noise” (SIN) test and test protocol to evaluate one’s “baseline” ability to understand speech-in-noise. This also allows valid measurement of this ability post-treatment (ie, after fitting the patient with amplification, FM, ALDs, cochlear implants, etc) to quantify improvement (ie, verification).
Although SIN test materials have been available for many years, concerns regarding test time and perhaps even a lack of belief that hearing aids can improve performance in noise have made clinical use of SIN tests rare. Ample evidence is now available to make speech-in-noise improvement a viable criterion for acceptable hearing aid fittings. Ideally, these protocols should require minimal clinical time during which rapport building, treatment justification, and improved device and setting selections occur (to improve speech-in-noise), thereby reducing total clinical time due to repeated office visits.
It’s All About Process
Kochkin3 reported successful patients treated via best practices required fewer office visits. Of note, the public perception of hearing devices is likely to substantially improve if devices are proven to improve speech perception in background noise—and of significant importance, it is difficult to argue against the need for professional services when “proof” of an appropriate hearing aid fitting is a recognized and a standard part of the hearing aid fitting protocol. Kochkin4 reported 4 million people who were likely to benefit from hearing aid amplification did not purchase hearing aids that year (2007) based on subjective reports from their friends and relatives.
Hearing aid fitting protocols to date are primarily designed to increase audibility with an emphasis on speech signals (ie, to assure that speech sounds are audible) without making loud sounds uncomfortably loud. Many protocols also attempt to increase the signal-to-noise ratio (ie, to increase the loudness of the intended speech signal relative to the loudness of the background noise) usually with the prescription of directional microphones.
Best practice guidelines incorporate more than a core fitting algorithm, which include DSL, NAL, and manufacturer-based proprietary fitting protocols that predetermine gain, output, compression factors, and frequency shaping. Indeed, best practice hearing aid fitting protocols include the selection of appropriate size, style, features, and processes with regard to the selected hearing aids. Best practices also extend to counseling and auditory rehabilitative strategies, as well as verification and validation measures to ensure the selections are delivering the performance changes intended by the process.
Unfortunately, for many professionals, hearing aid fitting protocols have previously been essentially “threshold-based” and are most often not verified nor validated by the professional. Indeed, contemporary estimates indicate only 1 in 4 fittings are verified via “real ear” probe microphone measures. Therefore, in this article, we address the need to verify and validate hearing aid fitting protocols, and we propose a simple and straightforward protocol to accomplish this goal.
Verification and Validation
Frankly, although speech-in-noise is the number-one complaint of the majority of people with hearing loss and the majority of people wearing hearing aids, speech-in-noise is rarely (if ever) tested in most offices. Indeed, verification and validation measures are rarely applied in clinical practice. Kochkin, Beck, Christensen, and colleagues5 reported over 50% of all dispensing offices own real ear measurement (REM) equipment, yet REM is used in approximately 25% of all adult hearing aid fittings—and the percentage of use is significantly less for behavioral validation measures.
The often-heard claim of “insufficient clinical time” to perform validation and verification is a myth refuted by recent evidence. Kochkin3 hypothesized the lack of REM use (verification) and behavioral confirmation of performance while wearing hearing aids (validation) increases the total number of office visits. Specifically, based on 533 office visits, Kochkin reported the combination of verification and validation protocols decreased office visits on average by 1.2 visits, which is a lot more professional time than would be taken by speech in noise measures, not to mention wasted time incurred by the patient.
Audiograms and Hearing Aid Fittings
Of note, behavioral audiograms are “diagnostic tools.” Audiograms were not designed to serve as the basis of hearing aid fittings or counseling. Indeed, the authors argue that audiograms should not be used as primary counseling tools, and threshold-based fitting algorithms should ideally serve only as a “starting point” with regard to the overall “amplitude protocol” (gain, compression kneepoint, compression threshold and ratio, etc). The amount of gain added (across commercially available and proprietary hearing aid fitting algorithms) via the hearing aid circuit is based on the behavioral threshold volunteered by the patient. Of course, voluntary behavioral thresholds can change daily and are influenced by multiple factors, including mood, motivation, tinnitus, attention, depression, otologic disease, background noise, and much more.
Of significant importance, the spectral resolution of modern amplification devices (across the audible spectrum) is substantially greater than the tested and measured frequency resolution of the audiogram (often limited to 6 or 10 data points at 250, 500, 1000, 2000, 4000, 6000 Hz; or 250, 500, 750, 1000, 1500, 2000, 3000, 4000, 6000, 8000 Hz). Level-dependent gain is the amplification method of choice in most modern hearing devices. However, concepts like “most comfortable loudness” and “preferred listening level” are certainly not directly correlated with threshold measurements, as terms like “soft” or “comfortable” apply to a range of input levels. Further, sensitivity for pure tones does not predict the ability to detect speech in background noise, and does not differentially identify (or even infer) the level of benefit possible with contemporary amplification technology.
Getting the Selection Process Right: Compelling Reasons to Test SIN
The only way to know we have defined and improved the single most common complaint (SIN) is to measure it at two moments in time: pre-treatment and post-treatment. Of note, pre-treatment might simply be an un-aided SIN measurement. However, pre-treatment might also be an aided measurement obtained with the patient’s previous amplification system, with an aim toward comparing the previous system to the modern amplification system.

|
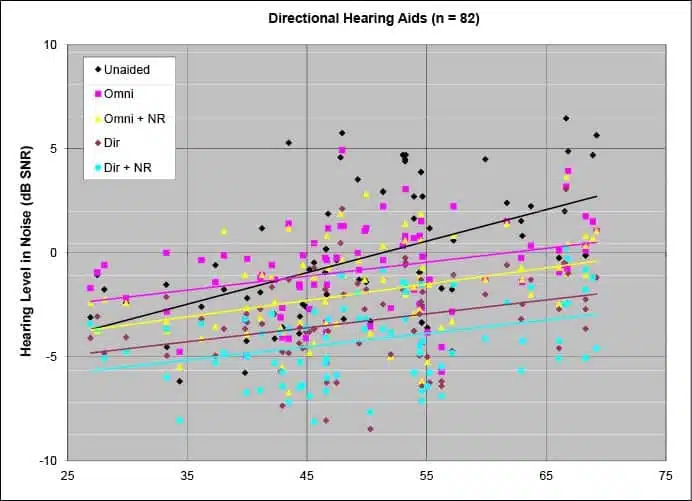
| Figure 1. HINT thresholds measured in diffuse noise for 82 subjects with mild to moderate, symmetric, sensorineural hearing loss testing unaided and aided in five hearing device configurations. The average lines suggest that users with mild losses don’t experience substantially better than the unaided condition until more features are activated. Adapted from Nilsson 2007.6 (Click image to enlarge) |
Figure 1 from Nilsson6 demonstrates data from 82 hearing-impaired listeners who were tested pre-and-post hearing aid fitting with the Hearing-in-Noise Test (HINT)7 in diffuse noise. The plot reveals several important points. First, unaided performance in noise is minimally predictive of aided performance in noise because substantial variability exists in individuals with the same hearing loss. Various hearing aid features, such as adaptive directionality and noise reduction, can improve performance (ie, lower scores on the y-axis) across a wide range of abilities. Of particular importance, listeners with good un-aided performance (those data points to the left in Figure 1) only show improved performance when all features that affect performance in noise, including directionality and noise reduction, are turned on.
People with “mild” hearing losses do not benefit from basic devices in noise and, indeed, do require advanced hearing aid circuitry—directionality, noise reduction, etc— to demonstrate improved speech perception in noise. Of note, people with more severe hearing losses demonstrate benefit from basic systems because “lack of audibility” (ie, their degree of hearing loss) is arguably the primary factor that degrades their performance in the first place. This audibility deficit does not allow them to perceive enough speech cues to identify speech. Simple amplification increases the audibility of speech sounds enough to allow them to perceive and identify additional speech sounds.
Conventional wisdom argues that complex and elaborate systems are only required for moderate, severe, and profound hearing losses. Figure 1 clearly shows this is incorrect. Indeed, this paradox represents a common clinical belief (ie, more processing is needed as hearing loss increases) and may be the reason appropriate technology is not always applied to patients who need and would benefit from it. However, these results (and similar) would not be known, unless SIN performance scores were obtained.
Therefore, although the behavioral audiogram is clearly an important diagnostic tool and serves as the foundation upon which audiologic diagnostics and rehabilitation are generally based, the audiogram should not serve as the primary foundation upon which hearing aid selections (or counseling) are based. Rather, in accordance with the number-one complaint of hearing-impaired people and people who wear hearing aids, we propose a simple addendum to validate and verify hearing aid fittings.8
A Proposal
SIN testing should be part of all hearing aid evaluations and diagnostic audiometric test protocols to document and objectify the most common complaint of all hearing-impaired people and hearing aid wearers. SIN testing to assess baseline performance serves to validate the patient’s primary complaint, and this same measure should be used later to demonstrate improvements in aided performance, attributable to the fitted hearing aids or the auditory rehabilitation protocol, or both. And, to be clear, fittings and/or aural rehabilitative strategies that do not deliver improved SIN performance should not be accepted.
Recommended Protocols
SIN testing should ideally involve commercially available test materials that have been standardized and are sensitive to changes in performance. SIN stimuli should come from recordings to reduce presentation variables, and SIN stimuli should involve sentences that are simple and relatively equal in context and equal in difficulty to assure sensitive and repeatable measurements. We agree with Taylor9 and recommend the following SIN tests:
- Hearing in Noise Test (HINT)10,11
- Words in Noise (WIN)12,13
- QuickSIN14,15
- Bamford-Kowal-Bench SIN (BKB-SIN)16-18
- Other SIN tests also may be appropriate.
Home-made SIN
For professionals unable to acquire commercially available test materials, “home made” adaptive SIN tests can be created simply and efficiently. The essential equipment involves two sound-field speakers and a 2-channel audiometer. In this approach, pre-recorded sentences are sent to one speaker (preferably from a CD player) via Channel 1, while background noise (white noise, pink noise, multi-talker babble, cafeteria noise, etc) is simultaneously sent to the second speaker via Channel 2. The two channels are presented at a reasonable MCL (most comfortable loudness level). Another option is to choose presentation levels that represent the real world (65 dBA represents an approximate conversational level for speech) or represent specific conditions of interest, such as soft, moderate, or loud noise to activate various signal processing automatics.
Before beginning the sentence test, noise should play long enough (eg, 10 seconds or so) for the automatic processing in the hearing aid to stabilize prior to speech materials being presented.
The SIN level is adapted to determine a bracketed SIN listening level. For example, if the background noise is presented at 60 dB (audiometer dial setting) and the sentences are delivered at 70 dB (audiometer dial setting), this represents a 10 dB SIN level. Assuming the patient repeats the sentences correctly and easily, the speech might be lowered to 65 dB, representing a 5 dB SIN level. If the patient again repeats the sentences correctly and easily, the next sentence presentation level might be 60 dB. Thus far, we have gone in 5 dB steps to approach the critical SIN level. Assuming the patient is unable to repeat the sentences at this newest and more challenging level (0 dB SIN), the sentence level may be raised and lowered (ie, bracketed) in 1 or 2 dB steps (depends on time constraints, fatigue, attention, desired accuracy, and other factors) until the protocol is concluded. We recommend bracketing in 2 dB steps to determine a pragmatic SIN level.
One might use 50% criteria (the patient is able to repeat half the words from the pre-recorded sentence) or one could use “successful” (repeats the entire sentence correctly) versus “unsuccessful” (is aware of the sentences but cannot repeat them). For the purpose of a “home-made” test, one should test 5 to 10 normal-hearing people, too, to practice and perfect the technique, and to establish “normal” SIN abilities for the particular equipment and location (for more information on creating a SIN test, see the 2013 AAA interview with Barbara E. Weinstein).19
Scoring can be accomplished either as an adaptive threshold (just like a clinical SRT, but using the sentence recordings relative to the noise level), or as a percent correct (as long as you avoid floor or ceiling effects). The absolute scores are less important than the change in score.
Interpretation of SIN results (ie, change in performance) is straightforward. A reasonably well-accepted rule of thumb is that a 1 dB change in SIN threshold equals an approximate 10% change in word recognition ability. For successful AR and/or successful hearing aid fittings, the SIN score will indicate an improved ability to understand speech in noise (the amount of benefit will vary from person to person).
It is noteworthy that people who do not demonstrate impaired listening in noise are unlikely to show improvement in their SIN scores. For example, some people with very mild sensorineural high frequency hearing loss may perform quite well in SIN tests, and therefore it is unrealistic to expect a significant change in their SIN test results (due to “ceiling effects”). However, for the majority of people who seek hearing aids to improve their listening skills, SIN testing will serve as an excellent barometer of success.
Summary
Because the primary complaint of all people with hearing loss and the primary complaint of all people wearing hearing aid amplification is speech-in-noise, we believe and advocate for SIN testing to become a standard part of every audiology diagnostic test battery. Indeed, establishing and documenting “un-aided” baseline SIN ability takes just a few minutes and facilitates direct comparison to an “aided” SIN score following aural rehabilitation and/or hearing aid fittings.

|

|
Douglas L. Beck, AuD, is director of professional relations at Oticon Inc, Somerset, NJ, and Michael Nilsson, PhD, is a senior research audiologist at Oticon A/S in Smoerum, Denmark. |
References
1. Taylor B. A proven strategy for addressing speech understanding in noise. Hearing Review. 2010;17(4)[Suppl]:4. Available at: /all-news/16973-a-proven-strategy-for-addressing-speech-understanding-in-noise
2. Kochkin S. MarkeTrak VIII: Consumer satisfaction with hearing aids is slowly increasing. Hearing Jour. 2010;63(1):19-32.
3. Kochkin S. MarkeTrak VIII: Reducing patient visits through verification and validation. Hearing Review. 2011;18(6):10-12. Available at: /products/17112-marketrak-viii-reducing-patient-visits-through-verification-amp-validation
4. Kochkin S. MarkeTrak VII: Obstacles to adult non-user adoption of hearing aids. Hear Jour. 2007;60(4):27-43.
5. Kochkin S, Beck DL, Christensen LA, Compton-Conley C, Kricos PB, Fligor BJ, McSpaden JB, Mueller HG, Nilsson MJ, Northern JL, Powers TA, Sweetow RW, Taylor B, Turner RG. MarkeTrak VIII: The impact of the hearing healthcare professional on hearing aid user success. Hearing Review. 2010;17(4):12-34. Available at: /practice-management/16967-marketrak-viii-the-impact-of-the-hearing-healthcare-professional-on-hearing-aid-user-success
6. Nilsson MJ. Speech intelligibility in noise with single-microphone noise reduction implemented in 9-, 16-, and 24-channel compression. Poster presentation at: Meeting of the Acoustical Society of America; 2007; Salt Lake City.
7. Nilsson M, Gelnett D, Sullivan J, Soli SD, Goldberg RL. Development of the Hearing in Noise Test for the measurement of speech reception thresholds in quiet and in noise. J Acoust Soc Am. 1992; 92(4):2385-2385.
8. Beck DL. Reflections on Change, Fitting Protocols, Counseling, Audiograms and More! IHS Soundboard 2013. Livonia, Mich: International Hearing Society; April.
9. Taylor B. Using speech-in-noise tests to make better hearing aid selection decisions. 2011. Available at: http://www.audiologyonline.com/articles/using-speech-in-noise-tests-832
10. Nilsson M, Soli SD, Sullivan JA. Development of the Hearing in Noise Test for the measurement of speech reception thresholds in quiet and in noise. J Acoust Soc Am. 1994;95(2):1085-99.
11. Wilson RH. Development of a speech-in-noise multitalker-babble paradigm to assess word-recognition performance. J Am Acad Audiol. 2003;14(9):453-470.
12. Wilson RH, Burks CA. Use of 35 words for evaluation of hearing loss in signal-to-babble ratio: a clinic protocol. J Rehabil Res Dev. 2005;42(6):839-852.
13. QuickSIN Speech-in-Noise Test, Version 1.3 [compact disc]. Elk Grove Village, Ill: Etymotic Research; 2001.
14. Killion MC, Niquette PA, Gudmundsen GI, Revit LJ, Banerjee S. Development of a quick speech-in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. J Acoust Soc Am. 2004;116:2395–2405.
15. Bench J, Kowal A, Bamford J. The BKB (Bamford-Kowal-Bench) Sentence Lists for partially-hearing children. Br J Audiol. 1979;13:108-112.
16. Etymotic Research. Bamford-Kowal-Bench Speech-in-Noise Test, Version 1.03 [compact disc]. Elk Grove Village, Ill: Etymotic Research; 2005.
17. Niquette P, Arcaroli J, Revit L, Parkinson A, Staller S, Skinner M, Killion M. Development of the BKB-SIN Test. Paper presented at: Annual meeting of the American Auditory Society; March 2003; Scottsdale, Ariz.
18. American Academy of Audiology (AAA) interview with Barbara E. Weinstein, PhD. In press. Will be available at www.audiology.org.
Recommended Reading
Aarts NL, Caffee CS. The accuracy and clinical usefulness of manufacturer predicted REAR values in adult hearing aid fittings. Hearing Review. 2005;12(12):16-22.
Aazh H, Moore BCJ, Prasher D. The accuracy of matching target insertion gains with open-fit hearing aids. Am J Audiol. 2012;21:175-180.
Abrams HB, Chisolm TH, McManus M, McArdle R. Initial fit approach versus verified prescription: comparing self-perceived hearing aid benefit. J Am Acad Audiol. 2012;23:768-778.
Beck DL, Duffy J. Visible speech—a patient-centered clinical tool. Hearing Review. www.hearingreview.com/issues/2007-01.asp
Nilsson MJ, Ghent RM, Bray VH, Harris R. Development of a test environment to evaluate performance of modern hearing aid features. J Am Acad Audiol. 2005;16(1):27-41.



